

Effect of angiotensin-converting enzyme inhibitors and receptor blockers on appropriate implantable cardiac defibrillator shock in patients with severe systolic heart failure (from the GRADE Multicenter Study)
- PMID: 25682436
- PMCID: PMC4363172
- DOI: 10.1016/j.amjcard.2015.01.020
Effect of angiotensin-converting enzyme inhibitors and receptor blockers on appropriate implantable cardiac defibrillator shock in patients with severe systolic heart failure (from the GRADE Multicenter Study)
Abstract
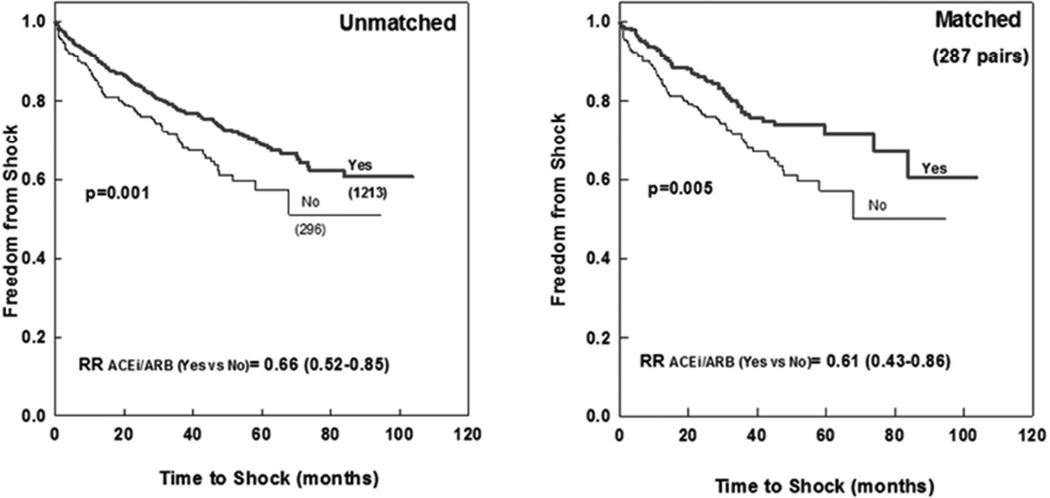
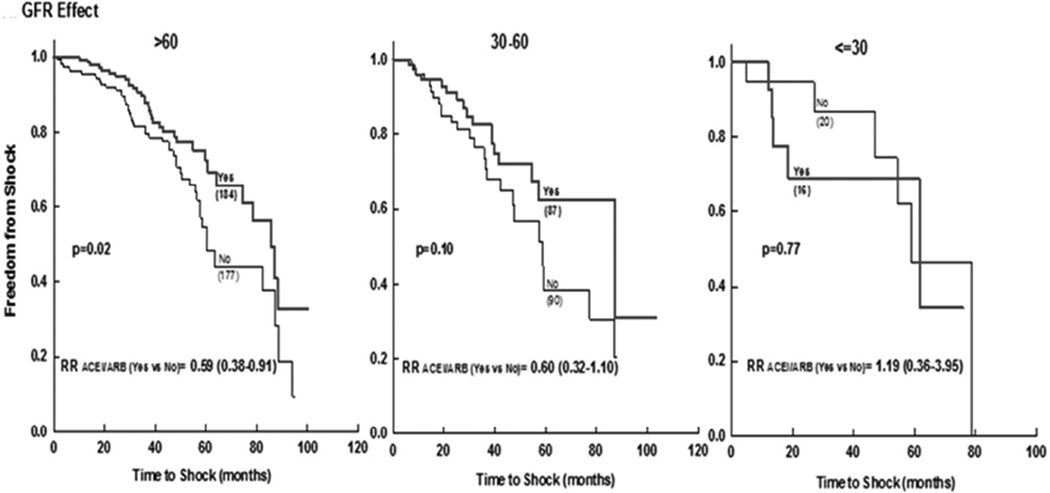
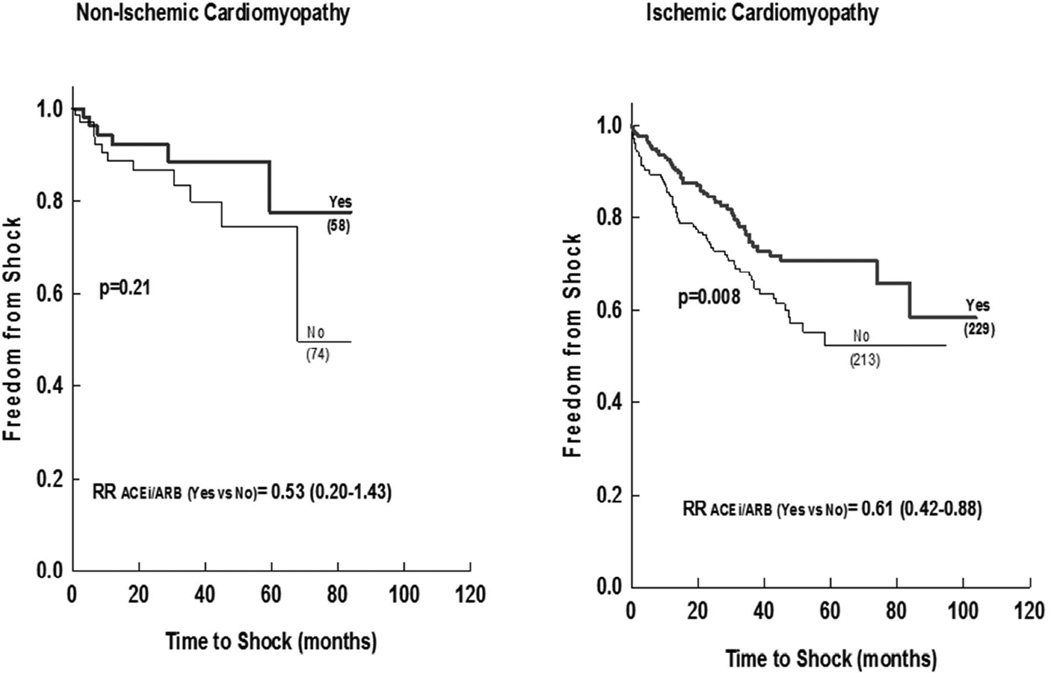
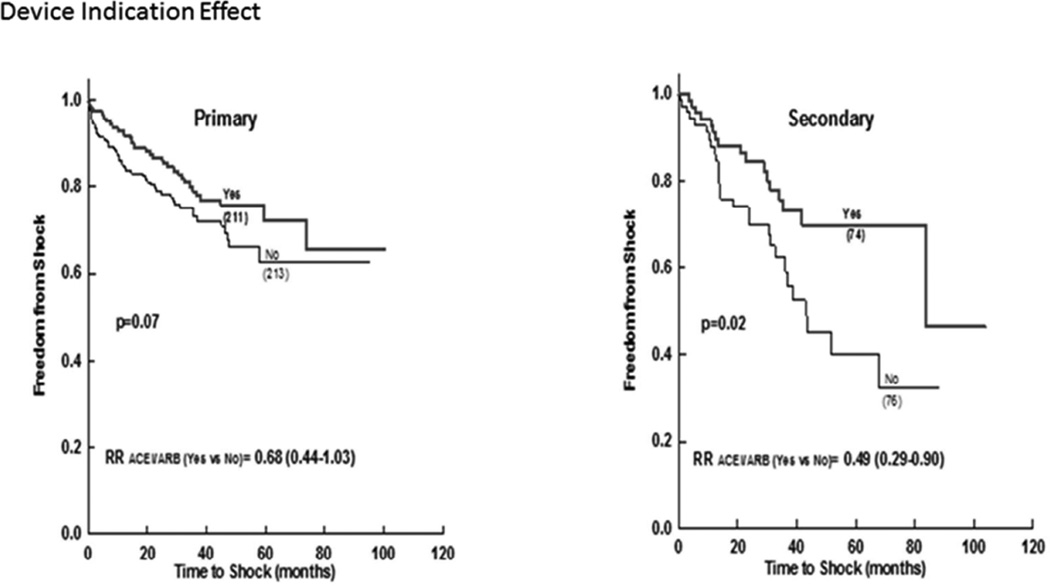
Sudden cardiac death (SCD) is a leading cause of mortality in patients with cardiomyopathy. Although angiotensin-converting enzyme inhibitors (ACEi) and angiotensin receptor blockers (ARBs) decrease cardiac mortality in these cohorts, their role in preventing SCD has not been well established. We sought to determine whether the use of ACEi or ARB in patients with cardiomyopathy is associated with a lower incidence of appropriate implantable cardiac defibrillator (ICD) shocks in the Genetic Risk Assessment of Defibrillator Events study that included subjects with an ejection fraction of ≤30% and ICDs. Treatment with ACEi/ARB versus no-ACEi/ARB was physician dependent. There were 1,509 patients (mean age [SD] 63 [12] years, 80% men, mean [SD] EF 21% [6%]) with 1,213 (80%) on ACEi/ARB and 296 (20%) not on ACEi/ARB. We identified 574 propensity-matched patients (287 in each group). After a mean (SD) of 2.5 (1.9) years, there were 334 (22%) appropriate shocks in the entire cohort. The use of ACEi/ARB was associated with lower incidence of shocks at 1, 3, and 5 years in the matched cohort (7.7%, 16.7%, and 18.5% vs 13.2%, 27.5%, and 32.0%; RR = 0.61 [0.43 to 0.86]; p = 0.005). Among patients with glomerular filtration rate (GFR) >60 and 30 to 60 ml/min/1.73 m(2), those on no-ACEi/ARB were at 45% and 77% increased risk of ICD shock compared with those on ACEi/ARB, respectively. ACEi/ARB were associated with significant lower incidence of appropriate ICD shock in patients with cardiomyopathy and GFR ≥30 ml/min/1.73 m(2) and with neutral effect in those with GFR <30 ml/min/1.73 m(2).
Trial registration: ClinicalTrials.gov NCT02045043.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
References
-
- Zipes DP, Wellens HJ. Sudden cardiac death. Circulation. 1998;98:2334–2351. - PubMed
-
- Schnee JM, Hsueh WA. Angiotensin II, adhesion, and cardiac fibrosis. Cardiovasc Res. 2000;46:264–268. - PubMed
-
- McEwan PE, Gray GA, Sherry L, Webb DJ, Kenyon CJ. Differential effects of angiotensin II on cardiac cell proliferation and intramyocardial perivascular fibrosis in vivo. Circulation. 1998;98:2765–2773. - PubMed
-
- Scott PA, Morgan JM, Carroll N, Murday DC, Roberts PR, Peebles CR, Harden SP, Curzen NP. The extent of left ventricular scar quantified by late gadolinium enhancement MRI is associated with spontaneous ventricular arrhythmias in patients with coronary artery disease and implantable cardioverter-defibrillators. Circ Arrhythm Electrophysiol. 2011;4:324–330. - PubMed
-
- Scott PA, Rosengarten JA, Murday DC, Peebles CR, Harden SP, Curzen NP, Morgan JM. Left ventricular scar burden specifies the potential for ventricular arrhythmogenesis: A LGE-CMR study. J Cardiovasc Electrophysiol. 2013;24:430–436. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
