

Final report of a phase II study of imatinib mesylate with hyper-CVAD for the front-line treatment of adult patients with Philadelphia chromosome-positive acute lymphoblastic leukemia
- PMID: 25682595
- PMCID: PMC4420214
- DOI: 10.3324/haematol.2014.118588
Final report of a phase II study of imatinib mesylate with hyper-CVAD for the front-line treatment of adult patients with Philadelphia chromosome-positive acute lymphoblastic leukemia
Abstract
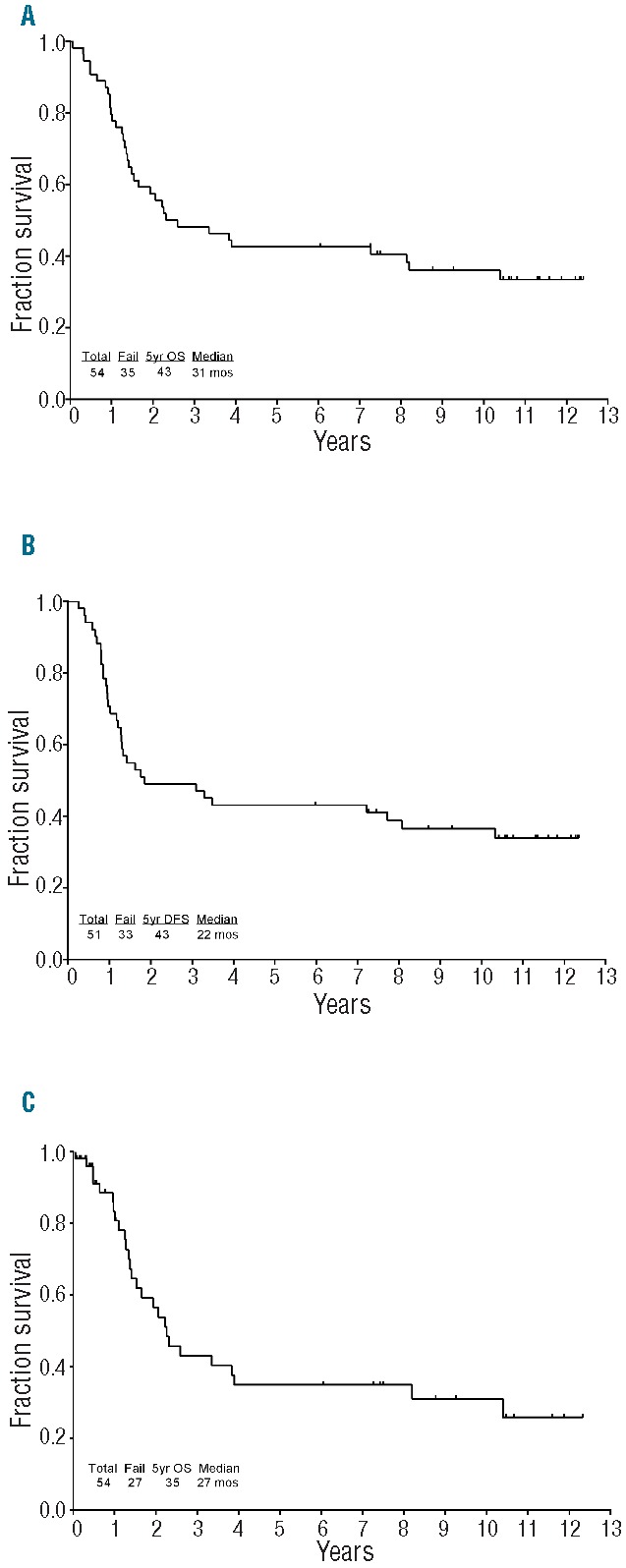
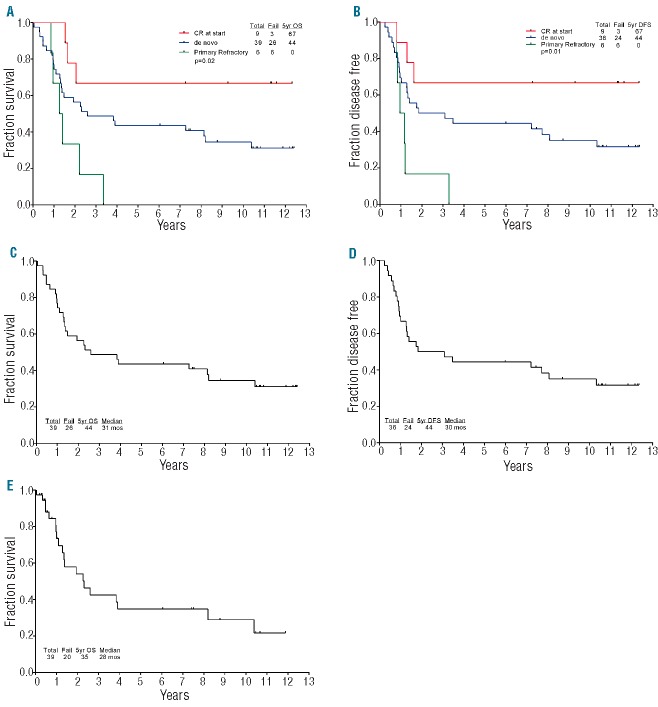
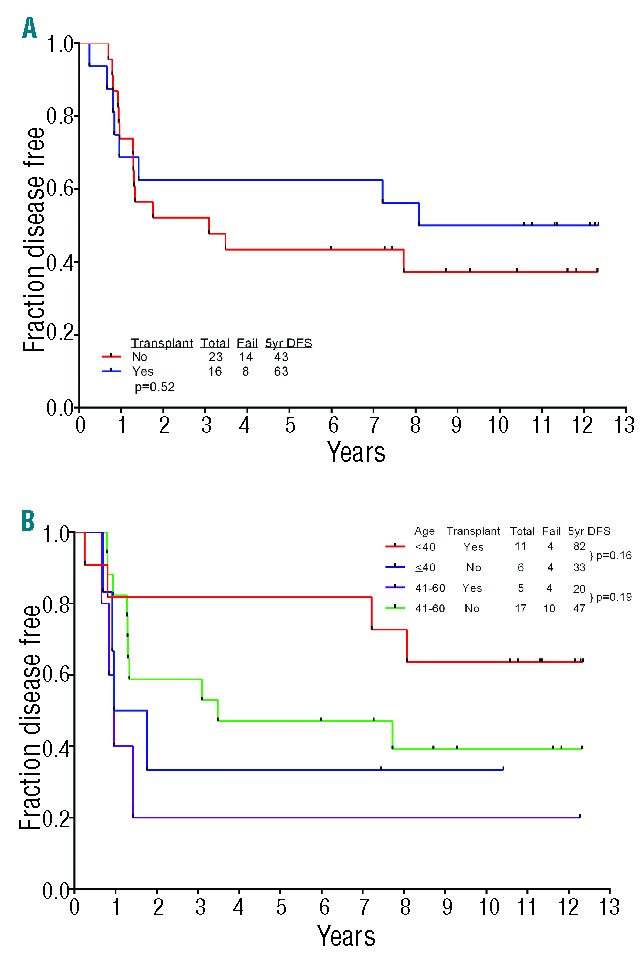
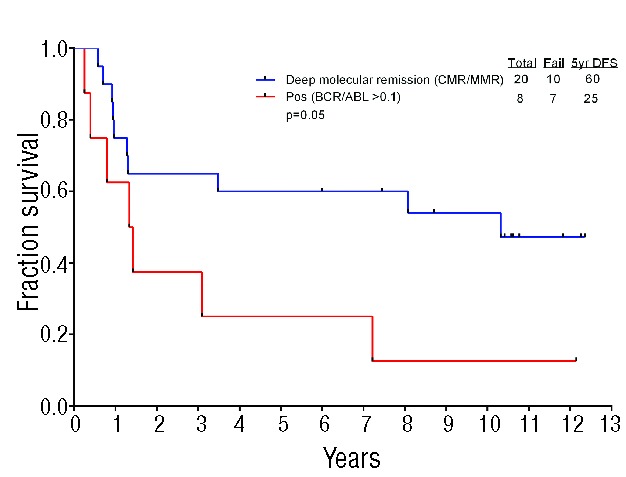
We have previously reported on the efficacy and tolerability of hyper-CVAD regimen (cyclophosphamide, vincristine, Adriamycin, and dexamethasone) and imatinib followed by imatinib-based consolidation/maintenance therapy in 20 patients with newly diagnosed Philadelphia-positive acute lymphoblastic leukemia. Here, we present the 13-year follow up of our study. Fifty-four patients with newly diagnosed Philadelphia-positive acute lymphoblastic leukemia were enrolled: 39 (72%) with de novo disease, 6 (11%) whose disease was primary refractory after induction (without a tyrosine kinase inhibitor), and 9 (17%) in complete remission after one course of induction therapy (without tyrosine kinase inhibitor). Forty-two (93%) of the 45 patients treated for active disease achieved complete remission, one achieved complete remission with incomplete recovery of platelets, one achieved partial remission and one died during induction. Nineteen (35%) patients are alive and 18 are in complete remission. The 5-year overall survival rate for all patients was 43%. Significant negative predictors of overall survival were age over 60 years, p190 molecular transcript, and active disease at enrollment. Sixteen (30%) patients underwent allogeneic stem cell transplantation. Median overall survival was not significantly greater for patients who underwent transplant. Patients with residual molecular disease at three months had improved complete remission duration with transplant. The median time to hematologic recovery and severe toxicities with combination were not significantly different from those observed with conventional chemotherapy. Only one patient discontinued therapy due to toxicity. HyperCVAD chemotherapy and imatinib is an effective regimen for Philadelphia-positive acute lymphoblastic leukemia. Transplant may not be indicated in all patients with Philadelphia-positive acute lymphoblastic leukemia. (clinicaltrials.gov identifier: NCT00038610).
Copyright© Ferrata Storti Foundation.
Figures
References
-
- Faderl S, Jeha S, Kantarjian HM. The biology and therapy of adult acute lymphoblastic leukemia. Cancer. 2003;98(7):1337–1354. - PubMed
-
- Bloomfield CD, Goldman AI, Alimena G, et al. Chromosomal abnormalities identify high-risk and low-risk patients with acute lymphoblastic leukemia. Blood. 1986; 67(2):415–420. - PubMed
-
- Moorman AV, Chilton L, Wilkinson J, Ensor HM, Bown N, Proctor SJ. A population-based cytogenetic study of adults with acute lymphoblastic leukemia. Blood. 2010; 115(2):206–214. - PubMed
-
- Burmeister T, Schwartz S, Bartram CR, et al. Patients’ age and BCR-ABL frequency in adult B-precursor ALL: a retrospective analysis from the GMALL study group. Blood. 2008;112(3):918–919. - PubMed
-
- Faderl S, Kantarjian HM, Thomas DA, et al. Outcome of Philadelphia chromosome-positive adult acute lymphoblastic leukemia. Leuk Lymphoma. 2000;36(3–4):263–273. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
