

Effectiveness and safety of lower dose prednisone for initial treatment of acute graft-versus-host disease: a randomized controlled trial
- PMID: 25682602
- PMCID: PMC4450631
- DOI: 10.3324/haematol.2014.118471
Effectiveness and safety of lower dose prednisone for initial treatment of acute graft-versus-host disease: a randomized controlled trial
Abstract
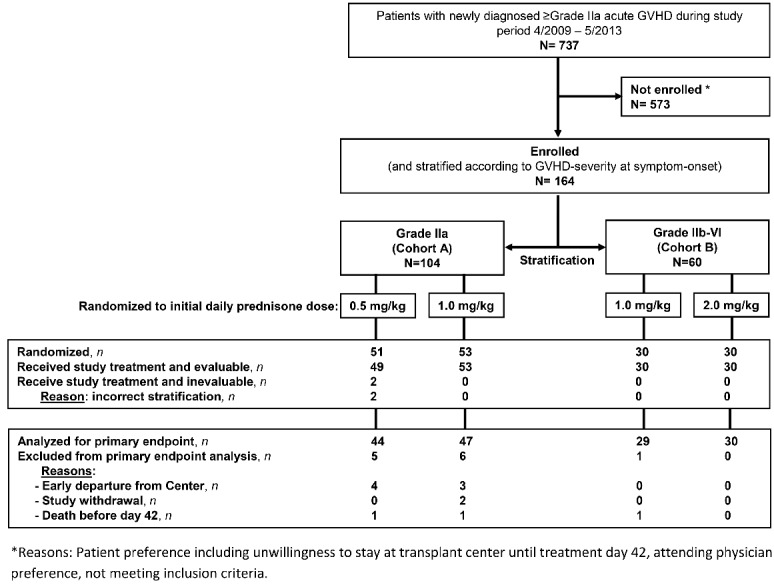
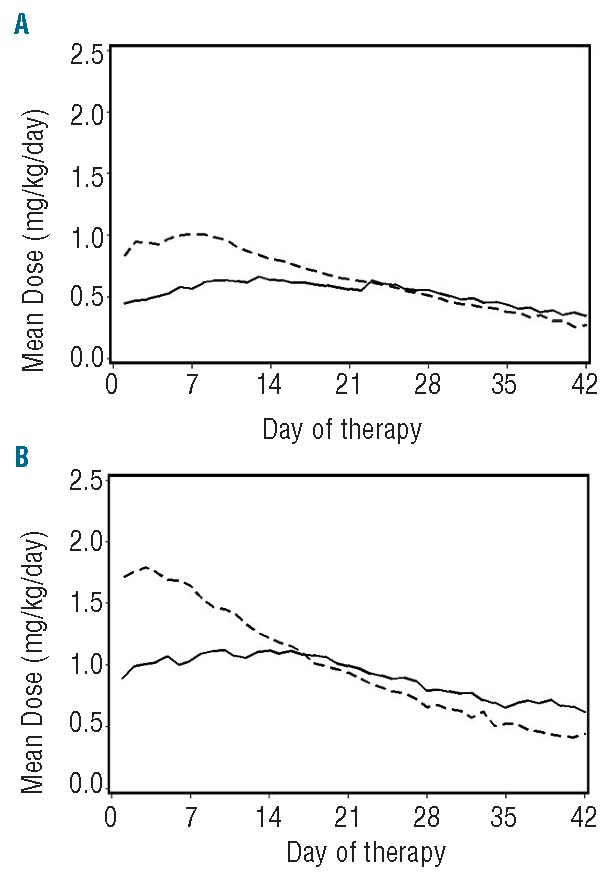
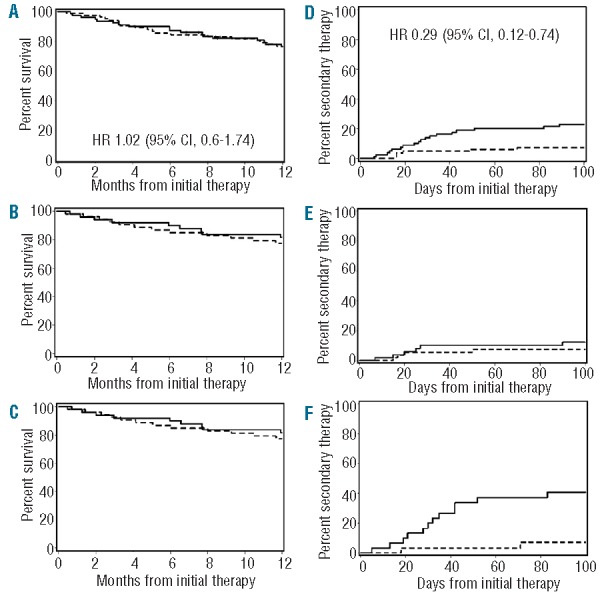
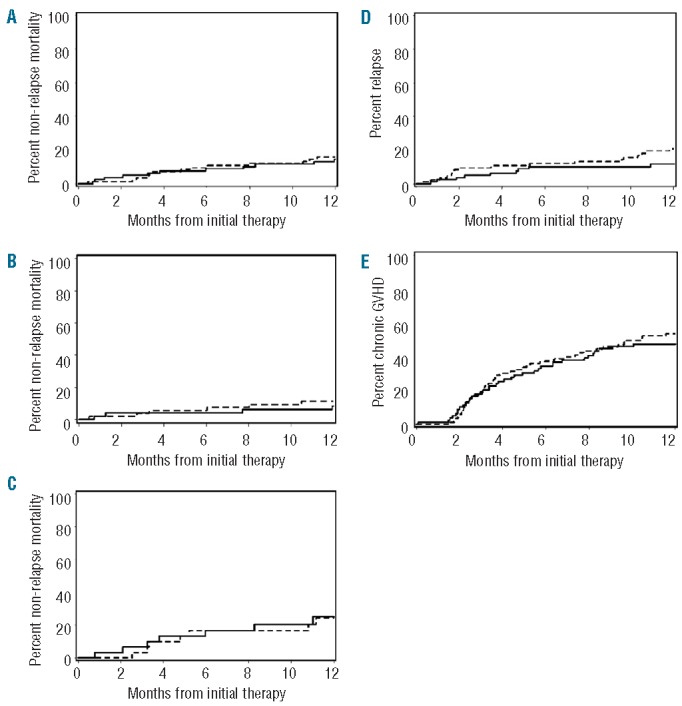
We conducted a phase III study to test the hypothesis that initial therapy with "lower dose" prednisone is effective and safe for patients with newly diagnosed acute graft-versus-host disease. We hypothesized that a 50% decrease in the initial dose of prednisone for treatment of acute graft-versus-host disease would suffice to control graft-versus-host disease without increasing the incidence of secondary treatment. Patients with grade IIa manifestations (upper gastrointestinal symptoms, stool volumes <1.0 L/day, rash involving <50% of the body surface, no hepatic dysfunction; n=102) were randomized to start treatment with prednisone at 1 mg/kg/day or 0.5 mg/kg/day. Those with grade IIb or higher manifestations (rash involving ≥50% of the body surface, stool volumes ≥1.0 L/day or hepatic involvement; n=62) were randomized to start treatment with prednisone at 2 mg/kg/day or 1 mg/kg/day. The primary study end point (a ≥33% relative reduction of the mean cumulative prednisone dose by day 42 after initial treatment with lower dose prednisone) was not reached. With a median follow up of 36 months (range 7-53), initial treatment with lower dose prednisone appeared to be effective for patients presenting with grade IIa manifestations since it did not increase the likelihood of requiring secondary immunosuppressive therapy. Further exploratory analyses suggested that for patients presenting with skin-predominant grade IIb or higher manifestations, initial treatment with lower dose prednisone was associated with an increased risk of requiring secondary immunosuppressive therapy (41% vs. 7%; P=0.001). In summary, initial treatment of newly diagnosed acute graft-versus-host disease with lower dose prednisone is effective. Within the statistical limitations of the study, results showed no suggestion that initial use of lower dose prednisone adversely affected survival.
Copyright© Ferrata Storti Foundation.
Figures
References
-
- Glucksberg H, Storb R, Fefer A, et al. Clinical manifestations of graft-versus-host disease in human recipients of marrow from HL-A-matched sibling donors. Transplantation. 1974;18(4):295–304. - PubMed
-
- Weisdorf D, Haake R, Blazar B, et al. Treatment of moderate/severe acute graft-versus-host disease after allogeneic bone marrow transplantation: An analysis of clinical risk features and outcome. Blood. 1990;75(4):1024–1030. - PubMed
-
- Shlomchik WD. Graft-versus-host disease (Review). Nat Rev Immunol. 2007;7(5):340–352. - PubMed
-
- Storb R, Deeg HJ, Whitehead J, et al. Methotrexate and cyclosporine compared with cyclosporine alone for prophylaxis of acute graft versus host disease after marrow transplantation for leukemia. N Engl J Med. 1986;314(12):729–735. - PubMed
-
- Martin PJ, Schoch G, Fisher L, et al. A retrospective analysis of therapy for acute graft-versus-host disease: initial treatment. Blood. 1990;76(8):1464–1472. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
