

The association of stillbirth with depressive symptoms 6-36 months post-delivery
- PMID: 25682858
- PMCID: PMC4371866
- DOI: 10.1111/ppe.12176
The association of stillbirth with depressive symptoms 6-36 months post-delivery
Abstract
Background: Stillbirths (≥ 20 weeks' gestation), which account for about 1 in 200 US pregnancies, may grieve parents deeply. Unresolved grief may lead to persistent depression.
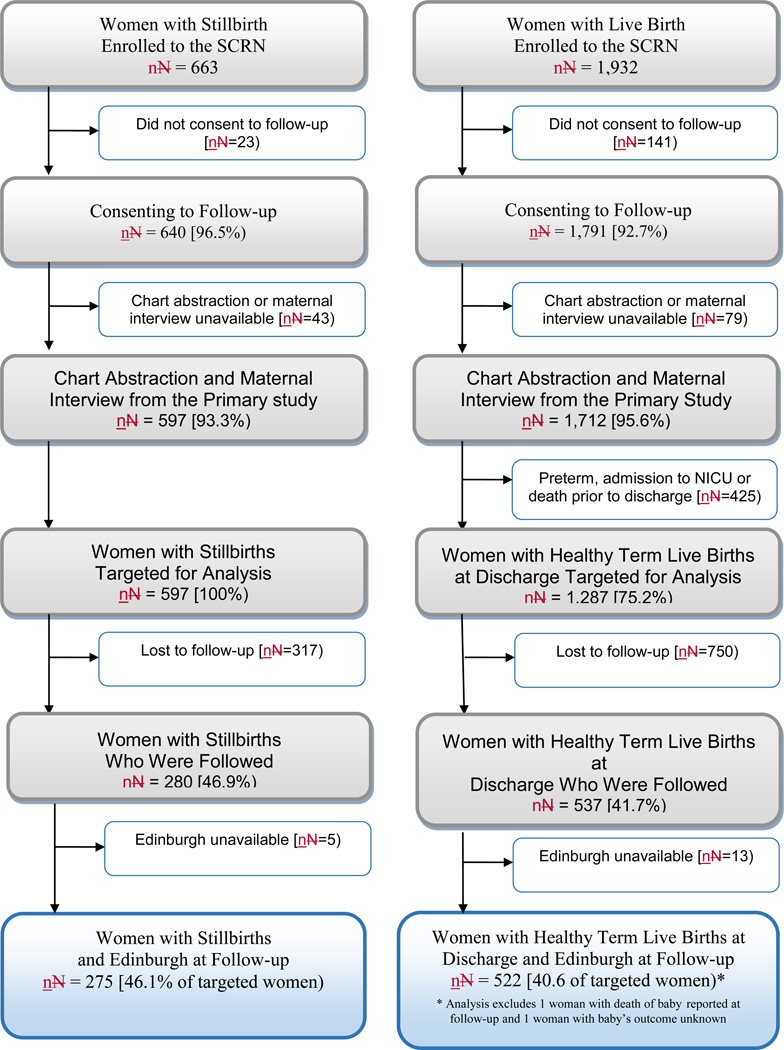
Methods: We compared depressive symptoms in 2009 (6-36 months after index delivery) among consenting women in the Stillbirth Collaborative Research Network's population-based case-control study conducted 2006-08 (n = 275 who delivered a stillbirth and n = 522 who delivered a healthy livebirth (excluding livebirths < 37 weeks, infants who had been admitted to a neonatal intensive care unit or who died). Women scoring > 12 on the Edinburgh Depression Scale were classified as currently depressed. Crude (cOR) and adjusted (aOR) odds ratios and 95% confidence intervals [CI] were computed from univariate and multivariable logistic models, with weighting for study design and differential consent. Marginal structural models examined potential selection bias due to low follow-up.
Results: Current depression was more likely in women with stillbirth (14.8%) vs. healthy livebirth (8.3%, cOR 1.90 [95% CI 1.20, 3.02]). However, after control for history of depression and factors associated with both depression and stillbirth, the stillbirth association was no longer significant (aOR 1.35 [95% CI 0.79, 2.30]). Conversely, for the 76% of women with no history of depression, a significant association remained after adjustment for confounders (aOR 1.98 [95% CI 1.02, 3.82]).
Conclusions: Improved screening for depression and referral may be needed for women's health care. Research should focus on defining optimal methods for support of women suffering stillbirth so as to lower the risk of subsequent depression.
Keywords: African Americans; Stillbirth; depression; follow-up studies; grief.
© 2015 John Wiley & Sons Ltd.
Figures
References
-
- MacDorman MF, Kirmeyer SE, Wilson EC. Fetal and perinatal mortality, United States, 2006. National Vital Statistics Reports. 2012;60(8) - PubMed
-
- Centers for Disease Control, Reproductive Statistics Branch, Division of Vital Statistics, NCHS. [Accessed June 30, 2014];User guide to the 2012 fetal death public use file. http://www.cdc.gov/nchs/data_access/Vitalstatsonline.htm.
-
- Neugebauer R, Kline J, Shrout P, Skodol A, O’Connor P, Geller PA, et al. Major depressive disorder in the 6 months after miscarriage. Journal of the American Medical Association. 1997;277:383–388. - PubMed
-
- Gold KJ, Johnson TR. Mothers at risk: maternal mental health outcomes after perinatal death. Obstetrics and Gynecology. 2014;123(Suppl 1):6S.
-
- Badenhorst W, Hughes P. Psychological aspects of perinatal loss. Best Practice and Research in Clinical Obstetrics and Gynaecology. 2007;21:249–259. http://www.sciencedirect.com/science/article/pii/S1521693406001416. - PubMed
Publication types
MeSH terms
Grants and funding
- U10 HD045925/HD/NICHD NIH HHS/United States
- U10 HD045952/HD/NICHD NIH HHS/United States
- U10-HD045925/HD/NICHD NIH HHS/United States
- U10 HD045955/HD/NICHD NIH HHS/United States
- U10-HD045955/HD/NICHD NIH HHS/United States
- U10 HD045944/HD/NICHD NIH HHS/United States
- U10-HD045952/HD/NICHD NIH HHS/United States
- U10 HD045953/HD/NICHD NIH HHS/United States
- U10-HD045954/HD/NICHD NIH HHS/United States
- U01 HD045954/HD/NICHD NIH HHS/United States
- UK10-HD045944/HD/NICHD NIH HHS/United States
- U10-HD045953/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
