

Distribution and clinical significance of tumour-associated macrophages in pancreatic ductal adenocarcinoma: a retrospective analysis in China
- PMID: 25684992
- PMCID: PMC4324348
- DOI: 10.3747/co.22.2150
Distribution and clinical significance of tumour-associated macrophages in pancreatic ductal adenocarcinoma: a retrospective analysis in China
Abstract
Background: We aimed to characterize the localization and prognostic significance of tumour-associated macrophages (tams) in pancreatic ductal adenocarcinoma (pdac).
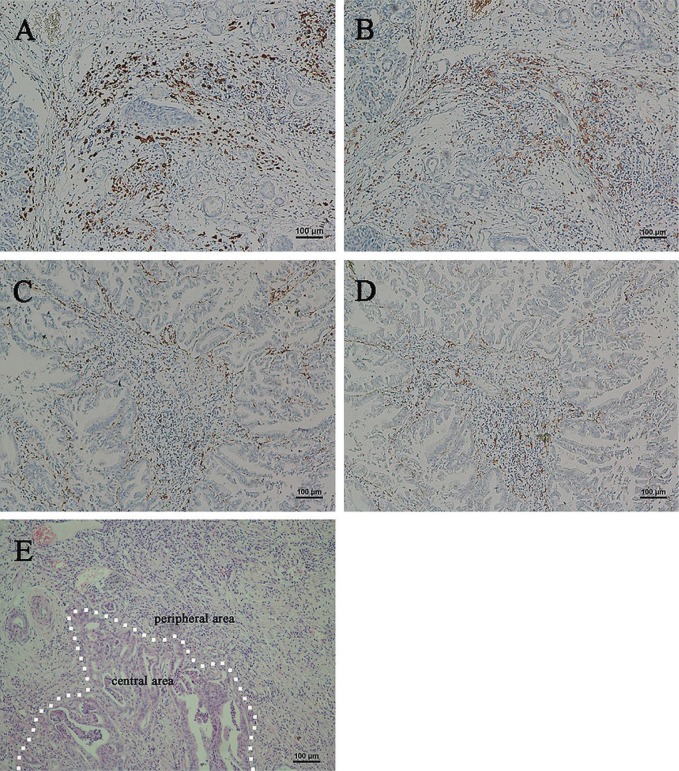
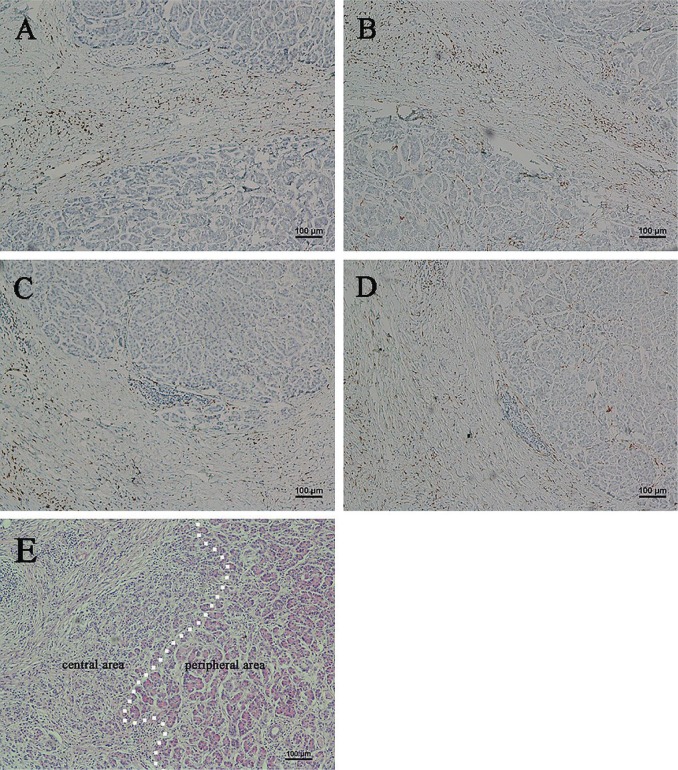
Methods: Tumour specimens from 70 patients with pdac and inflammatory specimens from 13 patients with chronic pancreatitis were collected and analyzed for tam and M2 macrophage counts by immunohistochemistry. Correlations between tam distributions and clinicopathologic features were determined.
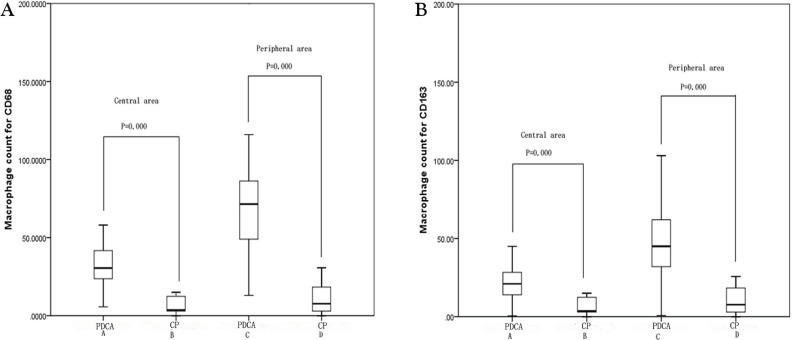
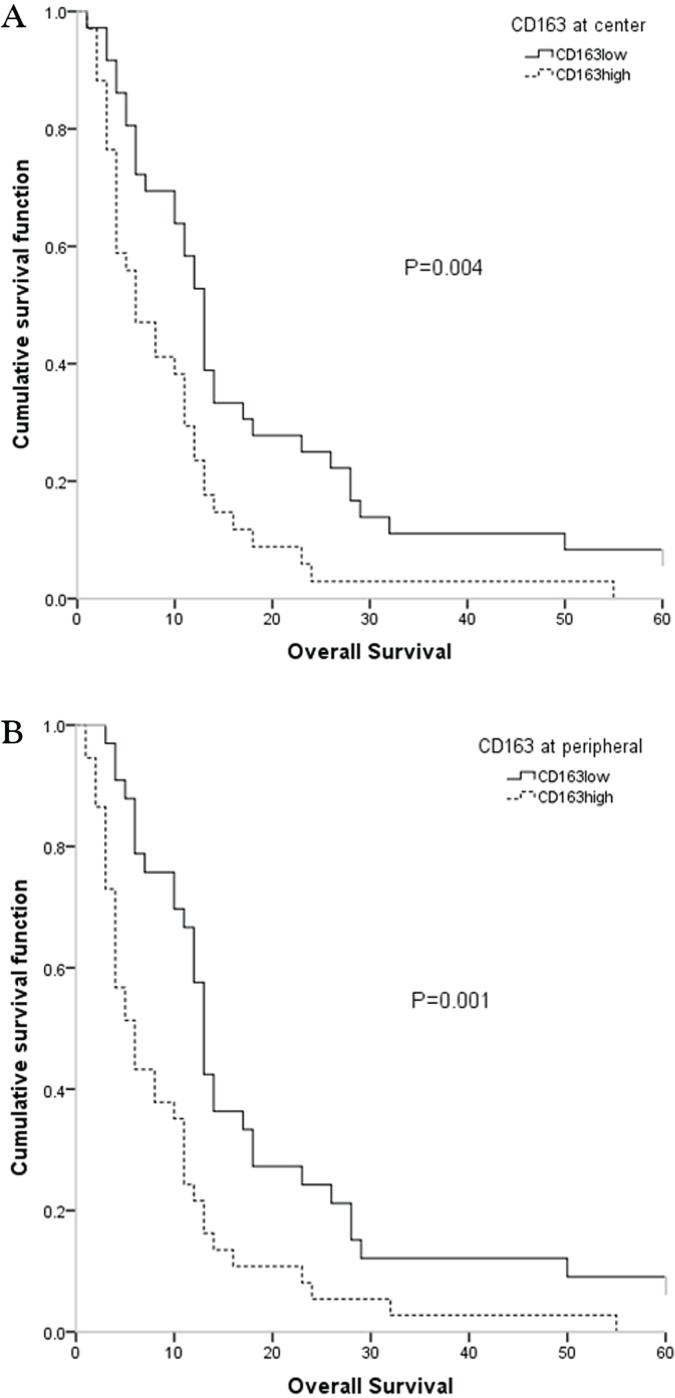
Results: Immunohistochemical analysis showed that tam and M2 macrophage counts were higher in tissues from pdac than from chronic pancreatitis. The tams and M2 macrophages both infiltrated more into peritumour. Both macrophage types were positively associated with lymph node metastasis (p = 0.041 for tams in peritumour, p = 0.013 for M2 macrophages in introtumour, p = 0.006 for M2 macrophage in peritumour). In addition, abdominal pain was significantly more frequent in pdac patients with a greater tams count. The survival rate was much lower in patients having high infiltration by M2 macrophages than in those having low infiltration.
Conclusions: The tam count might be associated with neural invasion in pdac, and M2 macrophages might play an important role in lymph node metastasis. Higher counts of either macrophage type were associated with increased risk of lymph node metastasis, and the M2 macrophage count could potentially be a marker for evaluating prognosis.
Keywords: Pancreatic cancer; lymph node metastasis; neural invasion; tumour-associated macrophages.
Figures
Similar articles
-
The CTCF/LncRNA-PACERR complex recruits E1A binding protein p300 to induce pro-tumour macrophages in pancreatic ductal adenocarcinoma via directly regulating PTGS2 expression.Clin Transl Med. 2022 Feb;12(2):e654. doi: 10.1002/ctm2.654. Clin Transl Med. 2022. PMID: 35184402 Free PMC article.
-
Identification of Transcriptomic Signatures of Pancreatic Ductal Adenocarcinoma-Derived Exosomes That Promote Macrophage M2 Polarization and Predict Prognosis: S100A9 Reveals Tumor Progression.Clin Med Insights Oncol. 2024 Mar 19;18:11795549241239042. doi: 10.1177/11795549241239042. eCollection 2024. Clin Med Insights Oncol. 2024. PMID: 38510315 Free PMC article.
-
Dual prognostic significance of tumour-associated macrophages in human pancreatic adenocarcinoma treated or untreated with chemotherapy.Gut. 2016 Oct;65(10):1710-20. doi: 10.1136/gutjnl-2015-309193. Epub 2015 Jul 8. Gut. 2016. PMID: 26156960
-
Prognostic Significance of Tumor-Associated Macrophage Content in Head and Neck Squamous Cell Carcinoma: A Meta-Analysis.Front Oncol. 2019 Jul 23;9:656. doi: 10.3389/fonc.2019.00656. eCollection 2019. Front Oncol. 2019. PMID: 31396482 Free PMC article.
-
Macrophage phenotype-switching in cancer.Eur J Pharmacol. 2022 Sep 15;931:175229. doi: 10.1016/j.ejphar.2022.175229. Epub 2022 Aug 21. Eur J Pharmacol. 2022. PMID: 36002039 Review.
Cited by
-
Targeting the tumor microenvironment in pancreatic ductal adenocarcinoma.Expert Rev Anticancer Ther. 2019 Jun;19(6):473-482. doi: 10.1080/14737140.2019.1622417. Epub 2019 May 31. Expert Rev Anticancer Ther. 2019. PMID: 31148495 Free PMC article. Review.
-
Combining sCD163 with CA 19-9 Increases the Predictiveness of Pancreatic Ductal Adenocarcinoma.Cancers (Basel). 2023 Jan 31;15(3):897. doi: 10.3390/cancers15030897. Cancers (Basel). 2023. PMID: 36765852 Free PMC article.
-
Single-cell image analysis reveals a protective role for microglia in glioblastoma.Neurooncol Adv. 2021 May 4;3(1):vdab031. doi: 10.1093/noajnl/vdab031. eCollection 2021 Jan-Dec. Neurooncol Adv. 2021. PMID: 34286275 Free PMC article.
-
The Fate of the Tumor in the Hands of Microenvironment: Role of TAMs and mTOR Pathway.Mediators Inflamm. 2016;2016:8910520. doi: 10.1155/2016/8910520. Epub 2016 Dec 15. Mediators Inflamm. 2016. PMID: 28074082 Free PMC article. Review.
-
The M2 phenotype of tumor-associated macrophages in the stroma confers a poor prognosis in pancreatic cancer.Tumour Biol. 2016 Jul;37(7):8657-64. doi: 10.1007/s13277-015-4741-z. Epub 2016 Jan 6. Tumour Biol. 2016. PMID: 26738860
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
