

New options for vascularized bone reconstruction in the upper extremity
- PMID: 25685100
- PMCID: PMC4317278
- DOI: 10.1055/s-0035-1544167
New options for vascularized bone reconstruction in the upper extremity
Abstract
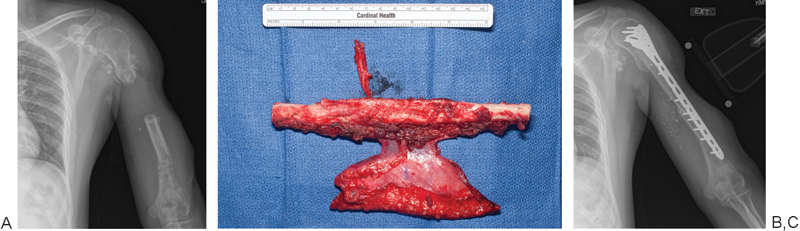
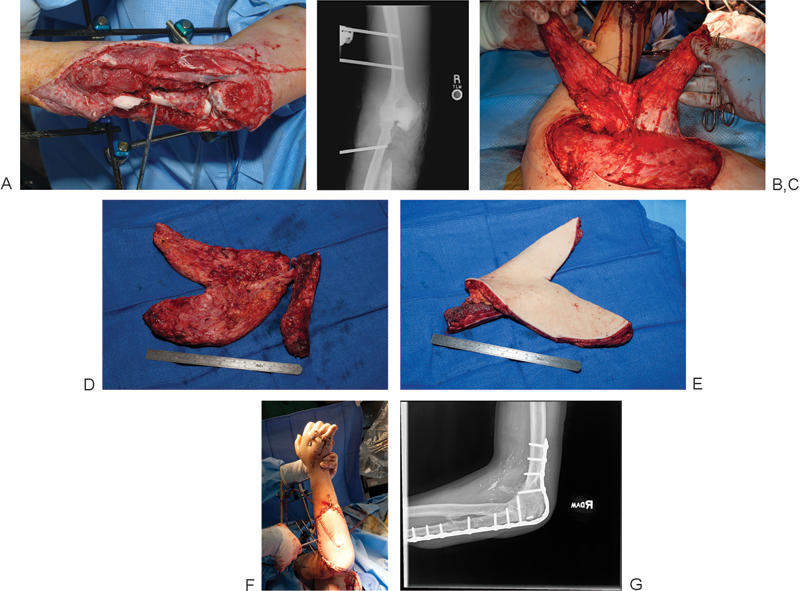
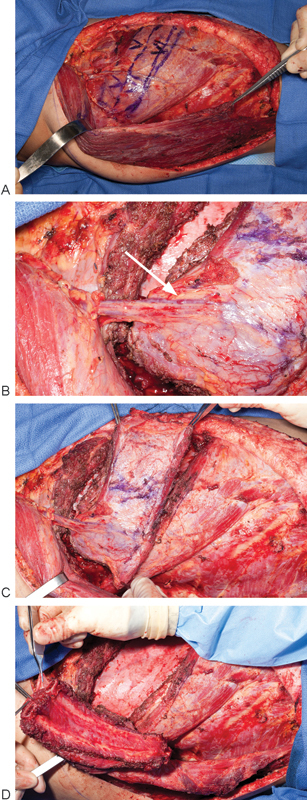
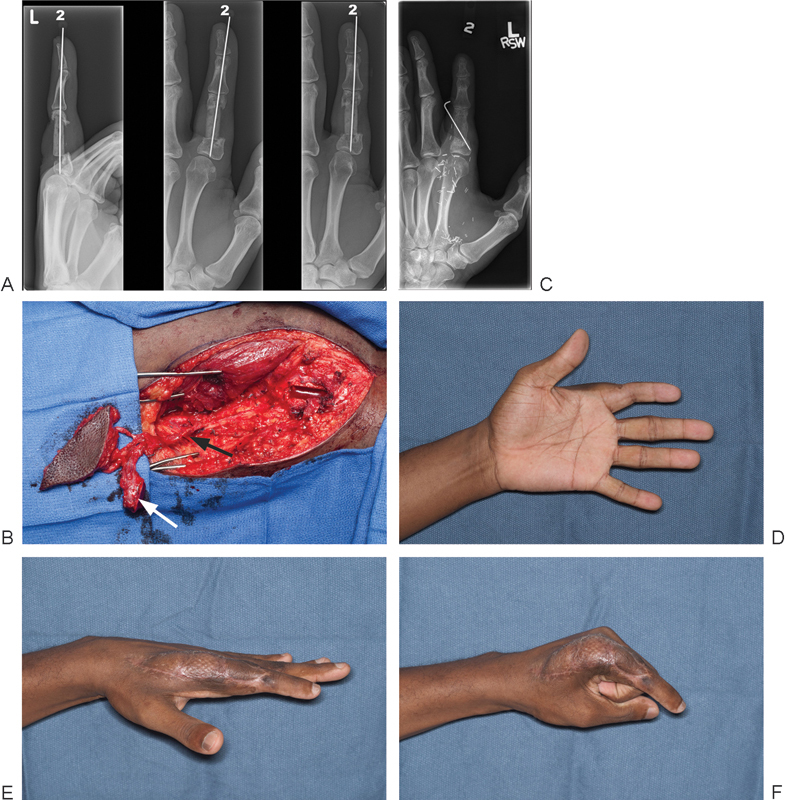
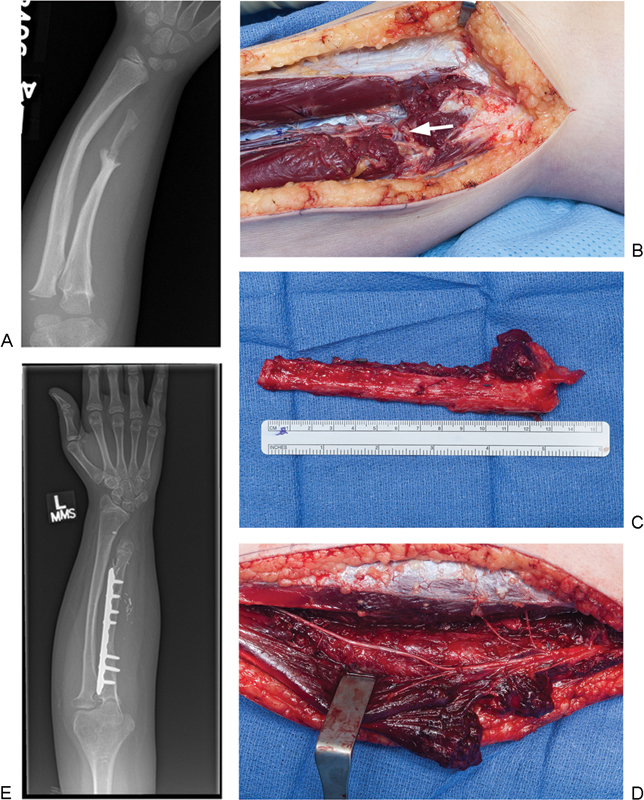
Originally described in the 1970s, vascularized bone grafting has become a critical component in the treatment of bony defects and non-unions. Although well established in the lower extremity, recent years have seen many novel techniques described to treat a variety of challenging upper extremity pathologies. Here the authors review the use of different techniques of vascularized bone grafts for the upper extremity bone pathologies. The vascularized fibula remains the gold standard for the treatment of large bone defects of the humerus and forearm, while also playing a role in carpal reconstruction; however, two other important options for larger defects include the vascularized scapula graft and the Capanna technique. Smaller upper extremity bone defects and non-unions can be treated with the medial femoral condyle (MFC) free flap or a vascularized rib transfer. In carpal non-unions, both pedicled distal radius flaps and free MFC flaps are viable options. Finally, in skeletally immature patients, vascularized fibular head epiphyseal transfer can provide growth potential in addition to skeletal reconstruction.
Keywords: bone graft; medial femoral condylar flap; vascularized bone graft; vascularized epiphyseal transfer; vascularized fibula.
Figures
References
-
- Wood M B, Cooney W P III, Irons G B Jr. Skeletal reconstruction by vascularized bone transfer: indications and results. Mayo Clin Proc. 1985;60(11):729–734. - PubMed
-
- Wood M B. Free vascularized bone transfers for nonunions, segmental gaps, and following tumor resection. Orthopedics. 1986;9(6):810–816. - PubMed
-
- de Boer H H, Wood M B. Bone changes in the vascularised fibular graft. J Bone Joint Surg Br. 1989;71(3):374–378. - PubMed
-
- Dell P C, Sheppard J E. Vascularized bone grafts in the treatment of infected forearm nonunions. J Hand Surg Am. 1984;9(5):653–658. - PubMed
-
- Taylor G I, Miller G D, Ham F J. The free vascularized bone graft. A clinical extension of microvascular techniques. Plast Reconstr Surg. 1975;55(5):533–544. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
