

doi: 10.1055/s-0035-1544171.
Upper extremity amputations and prosthetics
Affiliations
- PMID: 25685104
- PMCID: PMC4317270
- DOI: 10.1055/s-0035-1544171
Item in Clipboard
Upper extremity amputations and prosthetics
Semin Plast Surg.
2015 Feb.
Abstract
Upper extremity amputations are most frequently indicated by severe traumatic injuries. The location of the injury will determine the level of amputation. Preservation of extremity length is often a goal. The amputation site will have important implications on the functional status of the patient and options for prosthetic reconstruction. Advances in amputation techniques and prosthetic reconstructions promote improved quality of life. In this article, the authors review the principles of upper extremity amputation, including techniques, amputation sites, and prosthetic reconstructions.
Keywords: amputation; arm; finger; hand; prosthetic; upper extremity.
Figures
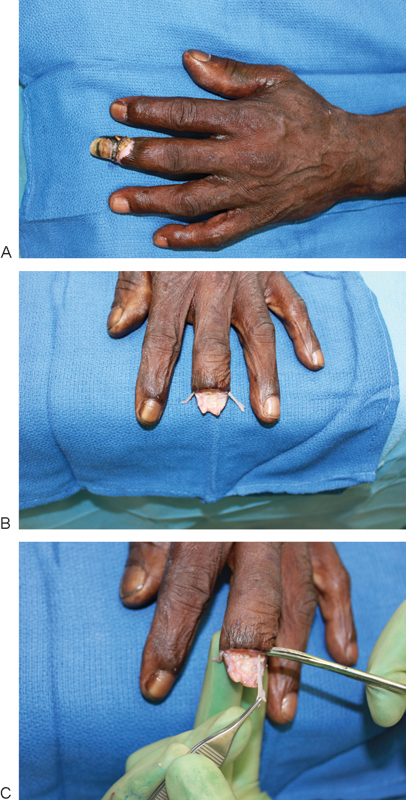
(A) Distal long finger to be amputated due to distal necrosis and osteomyelitis. (B) Digital nerves are carefully dissected prior to division. (C) Traction is applied to digital nerves during division to locate neuroma away from stump site.

(A) Crush injury to index finger necessitating partial amputation of distal phalanx. (B) Soft tissue closure is achieved with a local skin flap. (C) Proximal interphalangeal joint flexion is preserved by maintaining the insertion site of the flexor digitorum superficialis.
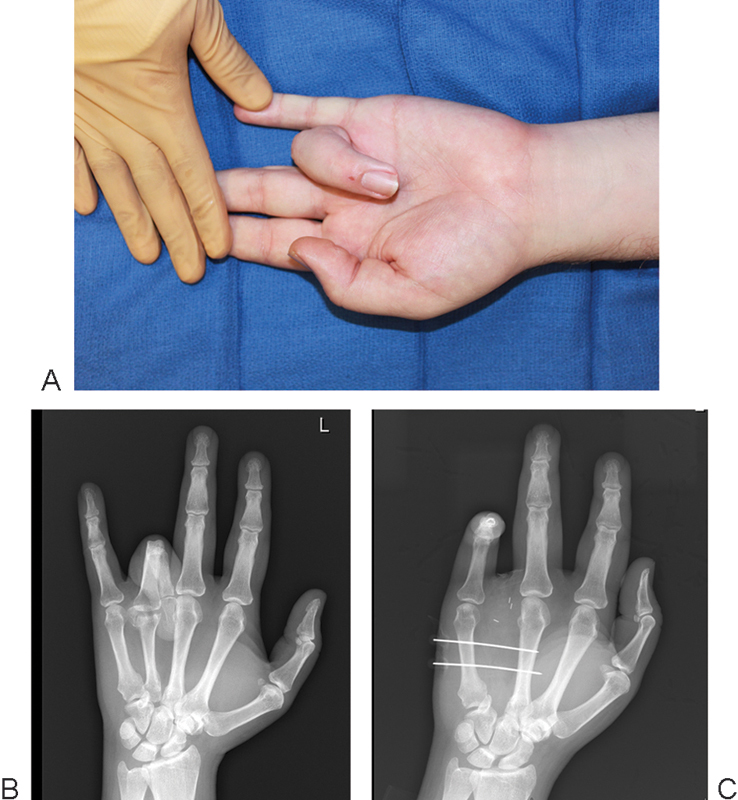
(A) Contracted insensate ring finger to be removed by ray amputation. (B) Radiograph demonstrating severe contraction deformity. (C) Radiograph after ring finger ray amputation. The third and fifth metacarpals were temporarily secured with K-wires to prevent widening of the web space during healing.
References
-
- Cioffi W G. Philadelphia, PA: Elsevier/Saunders; 2014. Upper extremity amputations; pp. 297–320.
-
- Cuccurullo S. New York, NY: Demos Medical; 2004. Physical Medicine and Rehabilitation Board Review.
-
- Prucz R B, Friedrich J B. Upper extremity replantation: current concepts. Plast Reconstr Surg. 2014;133(2):333–342. - PubMed
-
- Levine E A, Warso M A, McCoy D M, Das Gupta T K. Forequarter amputation for soft tissue tumors. Am Surg. 1994;60(5):367–370. - PubMed
-
- Luna-Ortiz K, Maafs-Molina E, Herrera-Gómez A, Barrera-Franco J L. Is there an indication for palliative surgical procedure of shoulder and upper limb malignancies? Cir Cir. 2003;71(2):102–106. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
