

β-cell dysfunction: Its critical role in prevention and management of type 2 diabetes
- PMID: 25685282
- PMCID: PMC4317303
- DOI: 10.4239/wjd.v6.i1.109
β-cell dysfunction: Its critical role in prevention and management of type 2 diabetes
Abstract
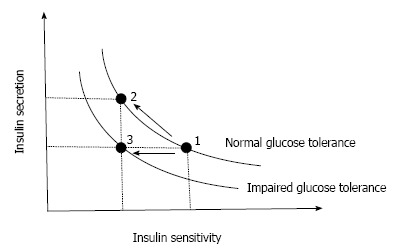
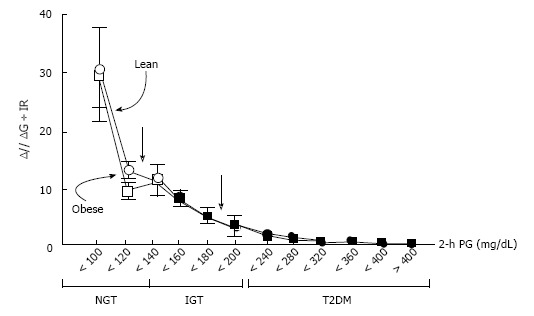
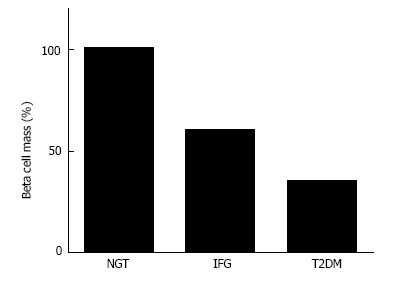
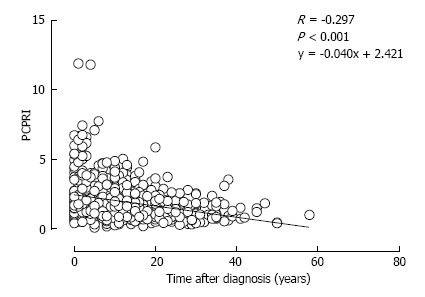
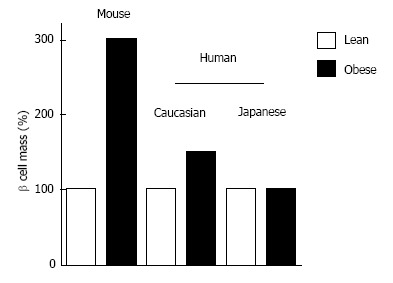
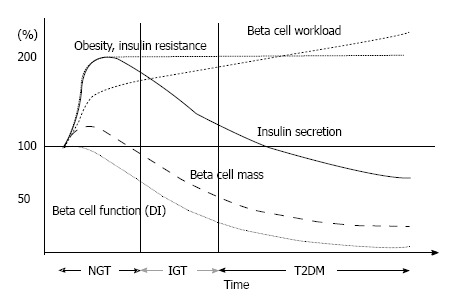
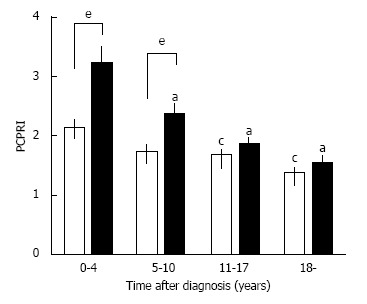
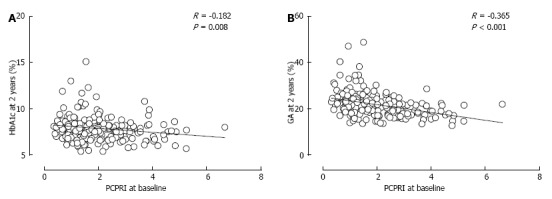
Type 2 diabetes (T2DM) is characterized by insulin resistance and β-cell dysfunction. Although, in contrast to type 1 diabetes, insulin resistance is assumed to be a major pathophysiological feature of T2DM, T2DM never develops unless β-cells fail to compensate insulin resistance. Recent studies have revealed that a deficit of β-cell functional mass is an essential component of the pathophysiology of T2DM, implying that β-cell deficit is a common feature of both type 1 and type 2 diabetes. β-cell dysfunction is present at the diagnosis of T2DM and progressively worsens with disease duration. β-cell dysfunction is associated with worsening of glycemic control and treatment failure; thus, it is important to preserve or recover β-cell functional mass in the management of T2DM. Since β-cell regenerative capacity appears somewhat limited in humans, reducing β-cell workload appears to be the most effective way to preserve β-cell functional mass to date, underpinning the importance of lifestyle modification and weight loss for the treatment and prevention of T2DM. This review summarizes the current knowledge on β-cell functional mass in T2DM and discusses the treatment strategy for T2DM.
Keywords: Insulin secretion; Prevention; Treatment; Type 2 diabetes; β-cell.
Figures
References
-
- Aguiree F, Brown A, Cho NH, Dahlquist G, Dodd S, Dunning T, Hirst M, Hwang C, Magliano D, Patterson C, et al. IDF Diabetes Atlas. IDF diabetes Atlas. 6th ed. Brussels, Belgium: International Diabetes Federation; 2013.
-
- Haffner SM, Lehto S, Rönnemaa T, Pyörälä K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med. 1998;339:229–234. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
