Efficacy of scrotal Doppler ultrasonography with the Valsalva maneuver, standing position, and resting-Valsalva ratio for varicocele diagnosis
- PMID: 25685302
- PMCID: PMC4325119
- DOI: 10.4111/kju.2015.56.2.144
Efficacy of scrotal Doppler ultrasonography with the Valsalva maneuver, standing position, and resting-Valsalva ratio for varicocele diagnosis
Abstract
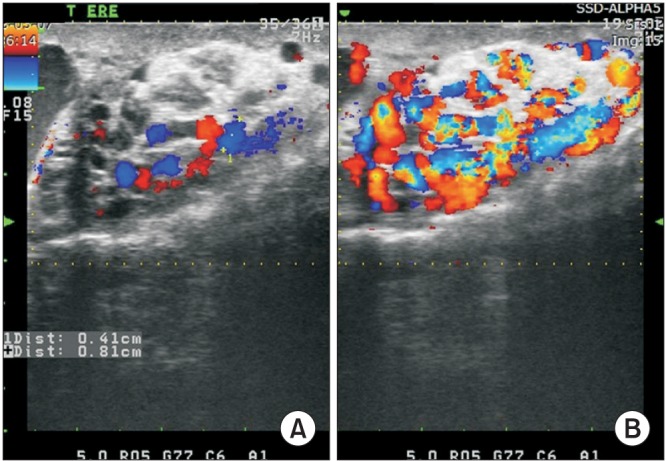
Purpose: To determine effectiveness of Valsalva maneuver and standing position on scrotal color Doppler ultrasound (CDU) for the varicocele diagnosis.
Materials and methods: We reviewed the physical examination and CDU finding in 87 patients who visited National Police Hospital from January 2011 to April 2014. Diameters of pampiniform plexus were measured bilaterally during resting and Valsalva maneuver in the supine position and standing position. We calculated the ratio of mean of maximal vein diameter (mMVD) during resting and Valsalva maneuver (resting-Valsalva ratio) and compared in the both position.
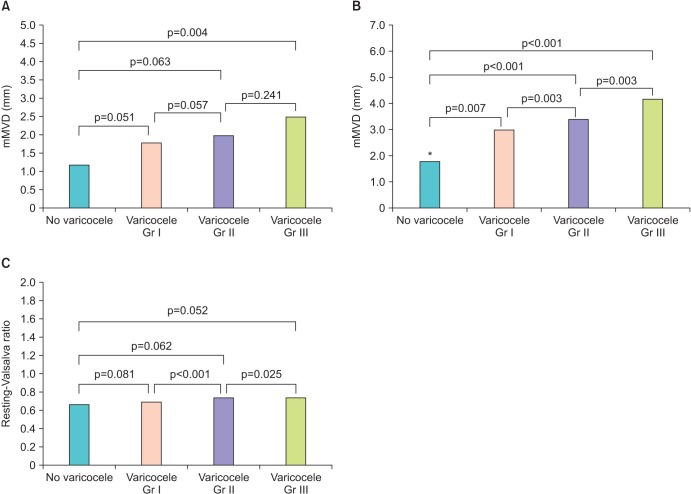
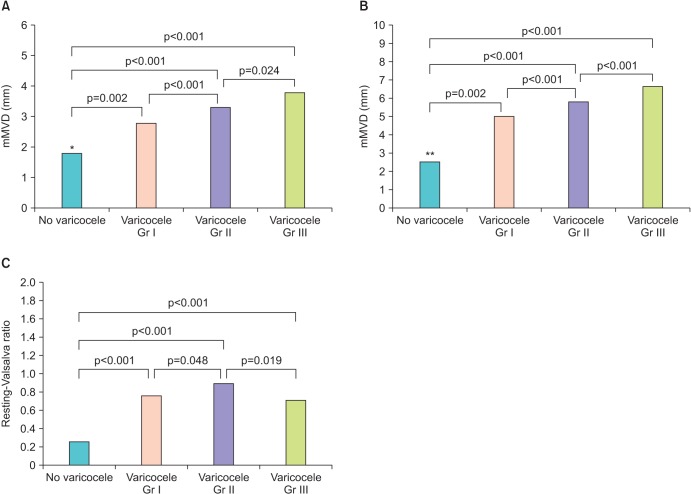
Results: In the resting and supine position, mMVD of varicocele testis units were 1.8 mm, 2.1 mm, 2.6 mm (grades I, II, III, respectively), and that of normal testis units (NTU) 1.2 mm. During Valsalva maneuver in the supine position, mMVD were 3.0 mm, 3.4 mm, 4.2 mm (grades I, II, III) vs 1.8 mm (NTU) (p=0.007, p<0.001, p<0.001, respectively). Average of resting-Valsalva ratio in the supine position were 0.69, 0.74, 0.74 (grades I, II, III) and 0.67 (NTU). Whereas in the resting and standing position, mMVD were 2.8 mm, 3.3 mm, 3.8 mm (grades I, II, III) and 1.8 mm (NTU) (p=0.002, p<0.001, p<0.001). During Valsalva maneuver in the standing position, mMVD were 5.0 mm, 5.8 mm, 6.6 mm (grades I, II, III) and 2.5 mm (NTU) (p=0.002, p<0.001, p<0.001). And average resting-Valsalva ratio were 0.76, 0.90, 0.71 (grades I, II, III) and 0.26 (NTU), which showed significant differences from all grades (p<0.001, p<0.001, p<0.001).
Conclusions: It is suggested that the standing position and Valsalva maneuver during CDU could improve diagnostic ability for varicocele. Resting-Valsalva ratio in the standing position could be a new diagnostic index for varicocele diagnosis using CDU.
Keywords: Doppler ultrasonography; Valsalva maneuver; Varicocele.
Conflict of interest statement
The authors have nothing to disclose.
Figures
Comment in
-
Editorial Comment.J Urol. 2021 Oct;206(4):1007-1008. doi: 10.1097/JU.0000000000001877.02. Epub 2021 Jul 23. J Urol. 2021. PMID: 34293922 No abstract available.
References
-
- Sigmund G, Gall H, Bahren W. Stop-type and shunt-type varicoceles: venographic findings. Radiology. 1987;163:105–110. - PubMed
-
- Cornud F, Belin X, Amar E, Delafontaine D, Helenon O, Moreau JF. Varicocele: strategies in diagnosis and treatment. Eur Radiol. 1999;9:536–545. - PubMed
-
- Arslan H, Sakarya ME, Atilla MK. Clinical value of power Doppler sonography in the diagnosis of varicocele. J Clin Ultrasound. 1998;26:229. - PubMed
-
- Greenberg SH. Varicocele and male fertility. Fertil Steril. 1977;28:699–706. - PubMed
-
- Cina A, Minnetti M, Pirronti T, Vittoria Spampinato M, Canade A, Oliva G, et al. Sonographic quantitative evaluation of scrotal veins in healthy subjects: normative values and implications for the diagnosis of varicocele. Eur Urol. 2006;50:345–350. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous