

Estimation of MERS-Coronavirus Reproductive Number and Case Fatality Rate for the Spring 2014 Saudi Arabia Outbreak: Insights from Publicly Available Data
- PMID: 25685622
- PMCID: PMC4322060
- DOI: 10.1371/currents.outbreaks.98d2f8f3382d84f390736cd5f5fe133c
Estimation of MERS-Coronavirus Reproductive Number and Case Fatality Rate for the Spring 2014 Saudi Arabia Outbreak: Insights from Publicly Available Data
Abstract
Background: The Middle East Respiratory Syndrome Coronavirus (MERS-CoV) was initially recognized as a source of severe respiratory illness and renal failure in 2012. Prior to 2014, MERS-CoV was mostly associated with sporadic cases of human illness, of presumed zoonotic origin, though chains of person-to-person transmission in the healthcare setting were reported. In spring 2014, large healthcare-associated outbreaks of MERS-CoV infection occurred in Jeddah and Riyadh, Kingdom of Saudi Arabia. To date the epidemiological information published by public health investigators in affected jurisdictions has been relatively limited. However, it is important that the global public health community have access to information on the basic epidemiological features of the outbreak to date, including the basic reproduction number (R0) and best estimates of case-fatality rates (CFR). We sought to address these gaps using a publicly available line listing of MERS-CoV cases.
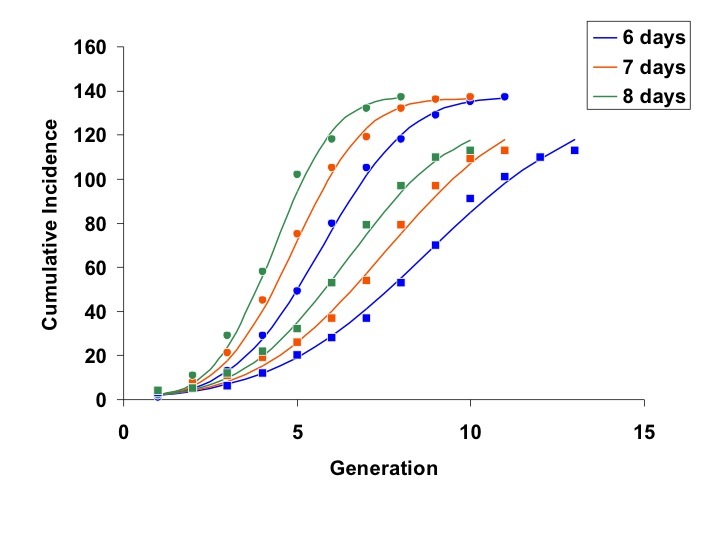
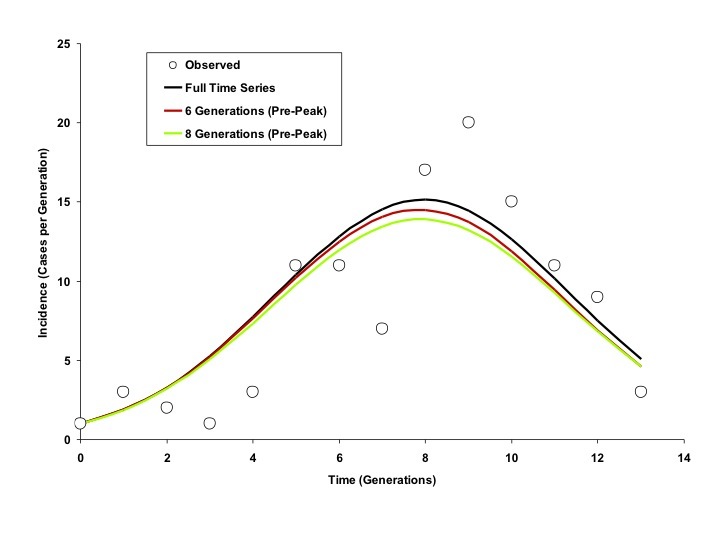
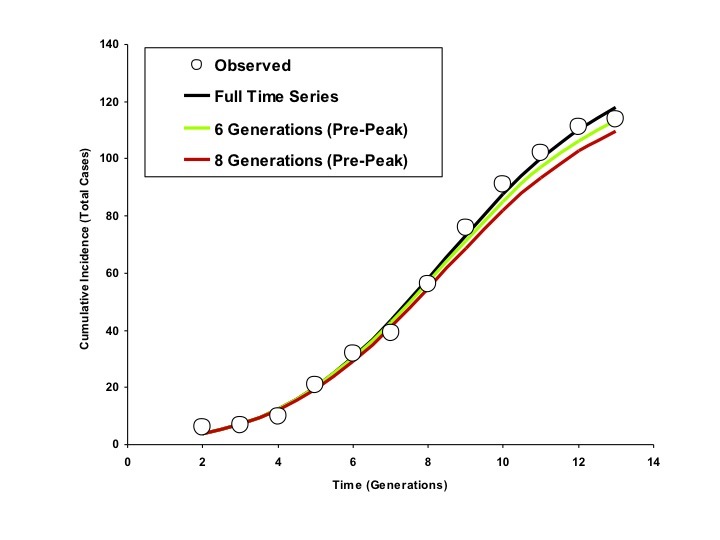
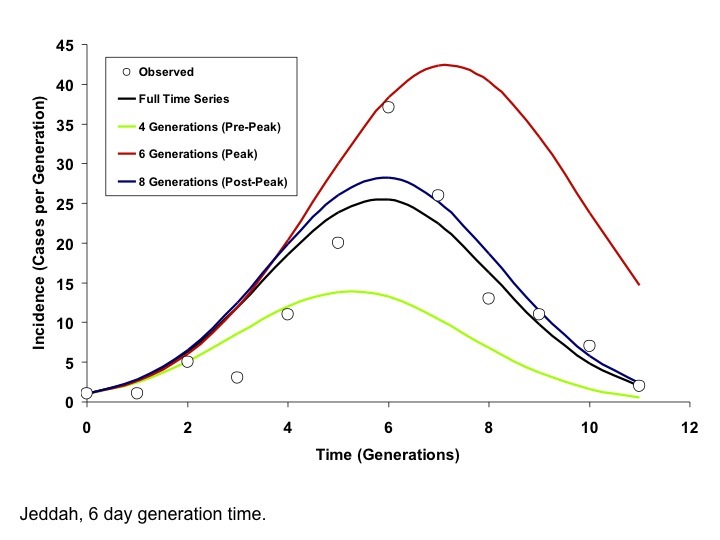
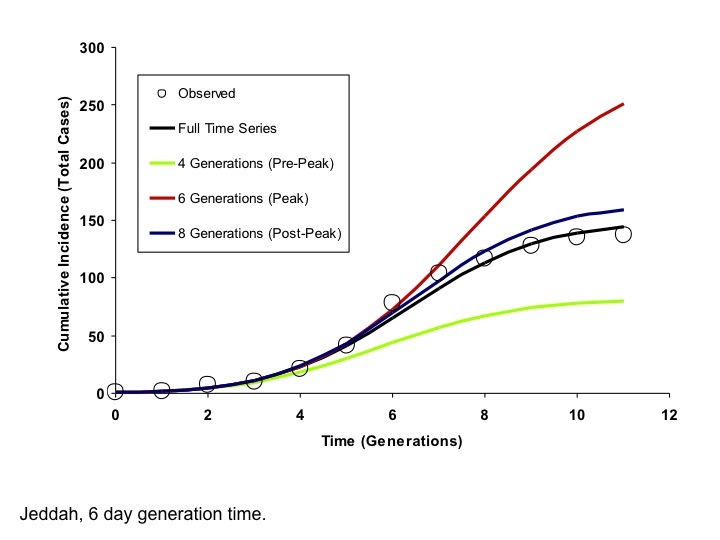
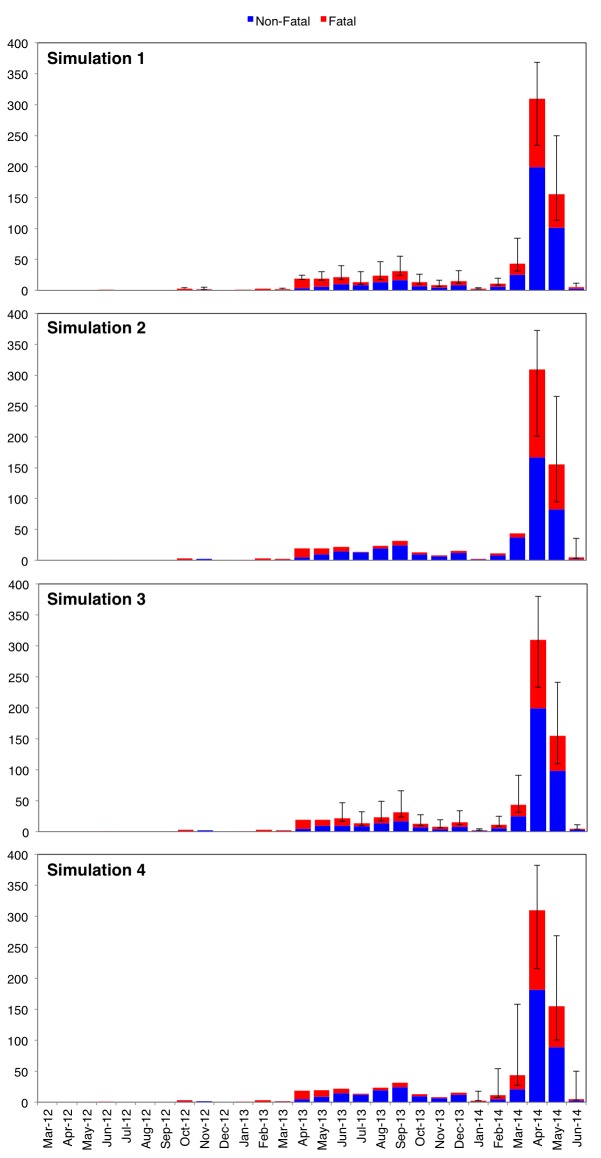
Methods: R0 was estimated using the incidence decay with exponential adjustment ("IDEA") method, while period-specific case fatality rates that incorporated non-attributed death data were estimated using Monte Carlo simulation.
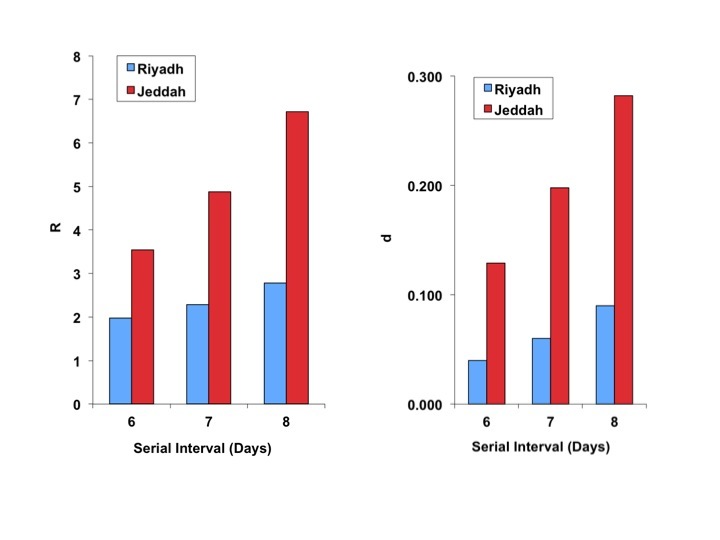
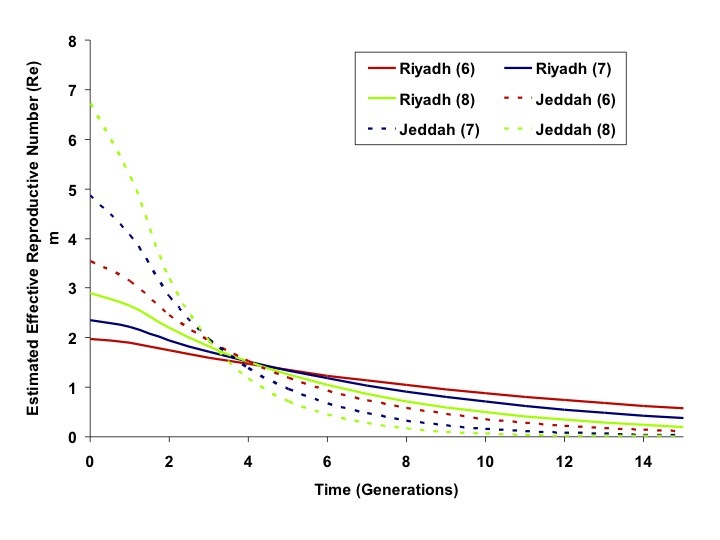
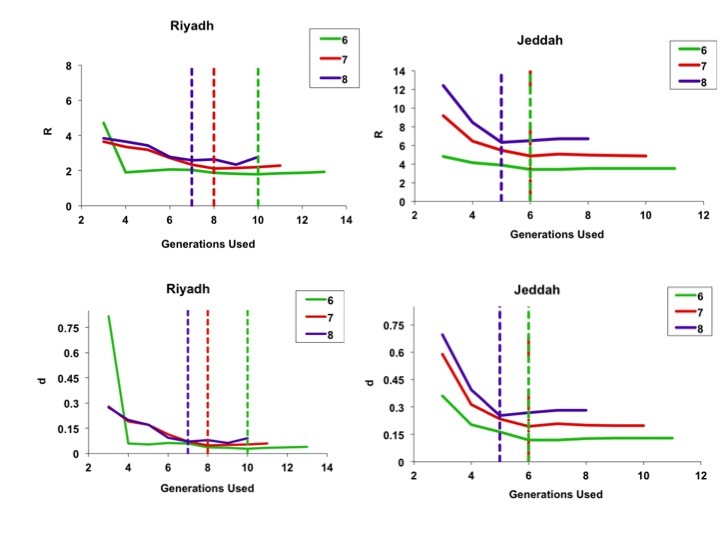
Results: 707 cases were available for evaluation. 52% of cases were identified as primary, with the rest being secondary. IDEA model fits suggested a higher R0 in Jeddah (3.5-6.7) than in Riyadh (2.0-2.8); control parameters suggested more rapid reduction in transmission in the former city than the latter. The model accurately projected final size and end date of the Riyadh outbreak based on information available prior to the outbreak peak; for Jeddah, these projections were possible once the outbreak peaked. Overall case-fatality was 40%; depending on the timing of 171 deaths unlinked to case data, outbreak CFR could be higher, lower, or equivalent to pre-outbreak CFR.
Conclusions: Notwithstanding imperfect data, inferences about MERS-CoV epidemiology important for public health preparedness are possible using publicly available data sources. The R0 estimated in Riyadh appears similar to that seen for SARS-CoV, but CFR appears higher, and indirect evidence suggests control activities ended these outbreaks. These data suggest this disease should be regarded with equal or greater concern than the related SARS-CoV.
Figures
References
-
- ProMED Mail, PRO/EDR> Novel coronavirus - Saudi Arabia: human isolate. ProMED-mail 2012; Sept 20: 20120920.1302733. http://www.promedmail.org. Accessed June 12, 2013.
-
- Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus AD, Fouchier RA. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. 2012 Nov 8;367(19):1814-20. PubMed PMID:23075143. - PubMed
-
- ProMED Mail, PRO/EDR> Novel coronavirus - Saudi Arabia (02): additional cases, RFI. ProMED-mail 2012; Sept 23: 20120923.1305931. http://www.promedmail.org. Bermingham A, Chand M, Brown C, et al. Severe respiratory illness caused by a novel coronavirus, in a patient transferred to the United Kingdom from the Middle East, Euro Surveill, 2012. 17(40): p. 20290. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
