

Modeling cardiac arrest and resuscitation in the domestic pig
- PMID: 25685718
- PMCID: PMC4326759
- DOI: 10.5492/wjccm.v4.i1.1
Modeling cardiac arrest and resuscitation in the domestic pig
Abstract
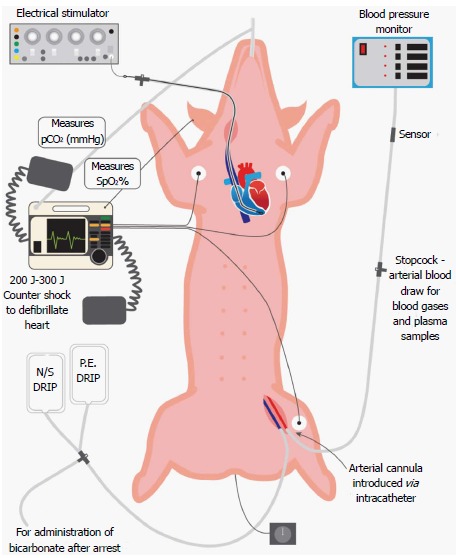
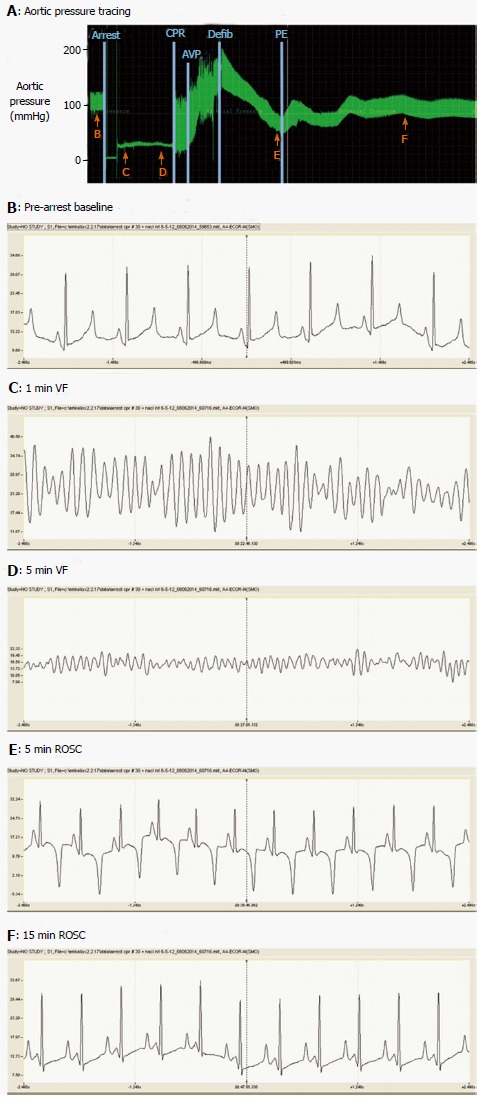
Cardiac arrest remains a leading cause of death and permanent disability worldwide. Although many victims are initially resuscitated, they often succumb to the extensive ischemia-reperfusion injury inflicted on the internal organs, especially the brain. Cardiac arrest initiates a complex cellular injury cascade encompassing reactive oxygen and nitrogen species, Ca(2+) overload, ATP depletion, pro- and anti-apoptotic proteins, mitochondrial dysfunction, and neuronal glutamate excitotoxity, which injures and kills cells, compromises function of internal organs and ignites a destructive systemic inflammatory response. The sheer complexity and scope of this cascade challenges the development of experimental models of and effective treatments for cardiac arrest. Many experimental animal preparations have been developed to decipher the mechanisms of damage to vital internal organs following cardiac arrest and cardiopulmonary resuscitation (CPR), and to develop treatments to interrupt the lethal injury cascades. Porcine models of cardiac arrest and resuscitation offer several important advantages over other species, and outcomes in this large animal are readily translated to the clinical setting. This review summarizes porcine cardiac arrest-CPR models reported in the literature, describes clinically relevant phenomena observed during cardiac arrest and resuscitation in pigs, and discusses numerous methodological considerations in modeling cardiac arrest/CPR. Collectively, published reports show the domestic pig to be a suitable large animal model of cardiac arrest which is responsive to CPR, defibrillatory countershocks and medications, and yields extensive information to foster advances in clinical treatment of cardiac arrest.
Keywords: Acidemia; Asphyxia; Cardiopulmonary resuscitation; Countershocks; Hyperoxia; Vasopressin; Ventricular fibrillation.
Figures
Similar articles
-
[Establishment of porcine model of prolonged cardiac arrest and cardiopulmonary resuscitation electrically induced by ventricular fibrillation].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017 Jun;29(6):536-541. doi: 10.3760/cma.j.issn.2095-4352.2017.06.012. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017. PMID: 28625244 Chinese.
-
Effects of potassium/lidocaine-induced cardiac standstill during cardiopulmonary resuscitation in a pig model of prolonged ventricular fibrillation.Acad Emerg Med. 2014 Apr;21(4):392-400. doi: 10.1111/acem.12348. Acad Emerg Med. 2014. PMID: 24730401
-
Extracorporeal resuscitation with carbon monoxide improves renal function by targeting inflammatory pathways in cardiac arrest in pigs.Am J Physiol Renal Physiol. 2019 Dec 1;317(6):F1572-F1581. doi: 10.1152/ajprenal.00241.2019. Epub 2019 Sep 4. Am J Physiol Renal Physiol. 2019. PMID: 31482730
-
Neuronal injury from cardiac arrest: aging years in minutes.Age (Dordr). 2014;36(4):9680. doi: 10.1007/s11357-014-9680-x. Epub 2014 Aug 8. Age (Dordr). 2014. PMID: 25104136 Free PMC article. Review.
-
Employing vasopressin during cardiopulmonary resuscitation and vasodilatory shock as a lifesaving vasopressor.Cardiovasc Res. 2001 Aug 15;51(3):529-41. doi: 10.1016/s0008-6363(01)00262-0. Cardiovasc Res. 2001. PMID: 11476743 Review.
Cited by
-
The Impact of a Modified Anaesthetic Protocol on Animal Survival and the Characteristics of Ventricular Arrhythmias in the Course of Acute Myocardial Infarction in a Domestic Pig Model.J Vet Res. 2022 Aug 30;66(3):435-447. doi: 10.2478/jvetres-2022-0046. eCollection 2022 Sep. J Vet Res. 2022. PMID: 36349138 Free PMC article.
-
A recommended preclinical extracorporeal cardiopulmonary resuscitation model for neurological outcomes: A scoping review.Resusc Plus. 2023 Jul 7;15:100424. doi: 10.1016/j.resplu.2023.100424. eCollection 2023 Sep. Resusc Plus. 2023. PMID: 37719942 Free PMC article.
-
Electrophysiological Monitoring of Brain Injury and Recovery after Cardiac Arrest.Int J Mol Sci. 2015 Oct 30;16(11):25999-6018. doi: 10.3390/ijms161125938. Int J Mol Sci. 2015. PMID: 26528970 Free PMC article. Review.
-
Disease-directed engineering for physiology-driven treatment interventions in neurological disorders.APL Bioeng. 2019 Oct 23;3(4):040901. doi: 10.1063/1.5117299. eCollection 2019 Dec. APL Bioeng. 2019. PMID: 31673672 Free PMC article.
-
A novel approach to assess cerebral and coronary perfusion after cardiac arrest.Intensive Care Med Exp. 2018 Oct 12;6(1):39. doi: 10.1186/s40635-018-0204-3. Intensive Care Med Exp. 2018. PMID: 30311018 Free PMC article.
References
-
- Kouwenhoven WB, Milnor WR, Knickerbocker GG, Chesnut WR. Closed chest defibrillation of the heart. Surgery. 1957;42:550–561. - PubMed
-
- Dezfulian C, Shiva S, Alekseyenko A, Pendyal A, Beiser DG, Munasinghe JP, Anderson SA, Chesley CF, Vanden Hoek TL, Gladwin MT. Nitrite therapy after cardiac arrest reduces reactive oxygen species generation, improves cardiac and neurological function, and enhances survival via reversible inhibition of mitochondrial complex I. Circulation. 2009;120:897–905. - PMC - PubMed
-
- Young GB. Clinical practice. Neurologic prognosis after cardiac arrest. N Engl J Med. 2009;361:605–611. - PubMed
-
- Heron M. Deaths: leading causes for 2009. Natl Vital Stat Rep. 2012;61:1–94. - PubMed
-
- Nolan JP, Lyon RM, Sasson C, Rossetti AO, Lansky AJ, Fox KA, Meier P. Advances in the hospital management of patients following an out of hospital cardiac arrest. Heart. 2012;98:1201–1206. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
