

An Endotoxin Tolerance Signature Predicts Sepsis and Organ Dysfunction at Initial Clinical Presentation
- PMID: 25685830
- PMCID: PMC4326653
- DOI: 10.1016/j.ebiom.2014.10.003
An Endotoxin Tolerance Signature Predicts Sepsis and Organ Dysfunction at Initial Clinical Presentation
Abstract
Background: Sepsis involves aberrant immune responses to infection, but the exact nature of this immune dysfunction remains poorly defined. Bacterial endotoxins like lipopolysaccharide (LPS) are potent inducers of inflammation, which has been associated with the pathophysiology of sepsis, but repeated exposure can also induce a suppressive effect known as endotoxin tolerance or cellular reprogramming. It has been proposed that endotoxin tolerance might be associated with the immunosuppressive state that was primarily observed during late-stage sepsis. However, this relationship remains poorly characterised. Here we clarify the underlying mechanisms and timing of immune dysfunction in sepsis.
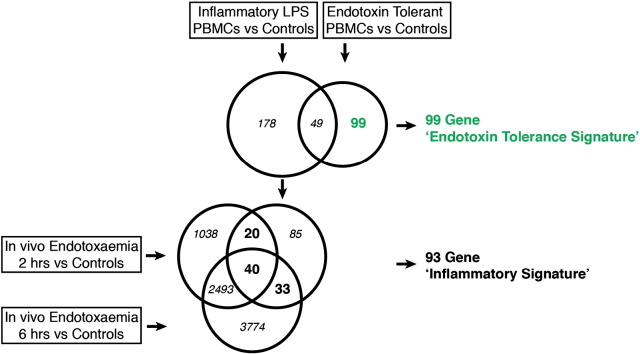
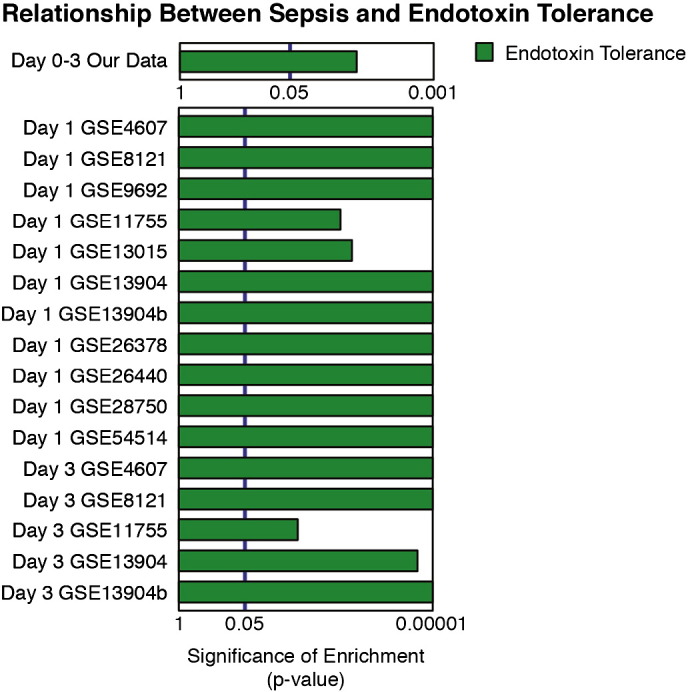
Methods: We defined a gene expression signature characteristic of endotoxin tolerance. Gene-set test approaches were used to correlate this signature with early sepsis, both newly and retrospectively analysing microarrays from 593 patients in 11 cohorts. Then we recruited a unique cohort of possible sepsis patients at first clinical presentation in an independent blinded controlled observational study to determine whether this signature was associated with the development of confirmed sepsis and organ dysfunction.
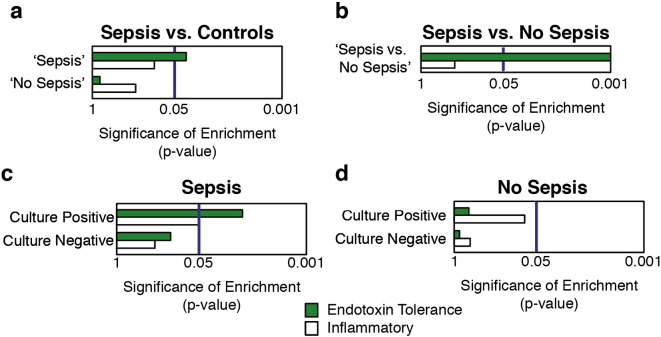
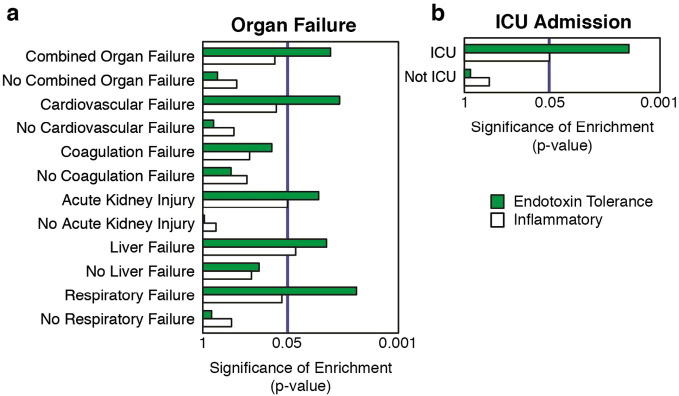
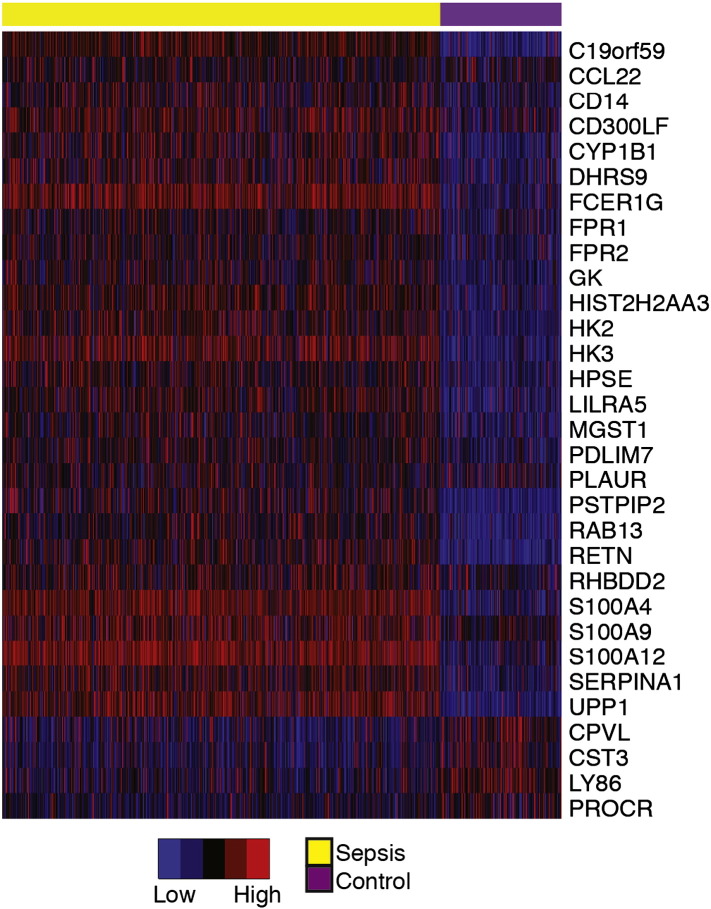
Findings: All sepsis patients presented an expression profile strongly associated with the endotoxin tolerance signature (p < 0.01; AUC 96.1%). Importantly, this signature further differentiated between suspected sepsis patients who did, or did not, go on to develop confirmed sepsis, and predicted the development of organ dysfunction.
Interpretation: Our data support an updated model of sepsis pathogenesis in which endotoxin tolerance-mediated immune dysfunction (cellular reprogramming) is present throughout the clinical course of disease and related to disease severity. Thus endotoxin tolerance might offer new insights guiding the development of new therapies and diagnostics for early sepsis.
Keywords: Cellular reprogramming; Diagnosis; Endotoxin tolerance; Immune dysfunction; Sepsis; Severe sepsis; Signature.
Figures
References
-
- Angus D., Linde-Zwirble W., Lidicker J., Clermont G., Carcillo J., Pinsky M. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit. Care Med. 2001;29(7):1303–1310. - PubMed
-
- Bone R.C., Balk R.A., Cerra F.B. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 2009. 1992;136(5 Suppl.):e28. - PubMed
-
- Buckley J.M., Wang J.H., Redmond H.P. Cellular reprogramming by gram-positive bacterial components: a review. J. Leukoc. Biol. 2006;80(4):731–741. - PubMed
-
- Calvano S.E., Xiao W., Richards D.R. A network-based analysis of systemic inflammation in humans. Nature. 2005;437(7061):1032–1037. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
