

Bilateral optic neuropathy and intraretinal deposits after pars plana vitrectomy in amyloidosis
- PMID: 25686071
- PMCID: PMC4363966
- DOI: 10.4103/0301-4738.151481
Bilateral optic neuropathy and intraretinal deposits after pars plana vitrectomy in amyloidosis
Erratum in
-
Bilateral optic neuropathy and intraretinal deposits after pars plana vitrectomy in amyloidosis: Erratum.Indian J Ophthalmol. 2015 Apr;63(4):365. doi: 10.4103/0301-4738.158111. Indian J Ophthalmol. 2015. PMID: 26044489 Free PMC article. No abstract available.
Abstract
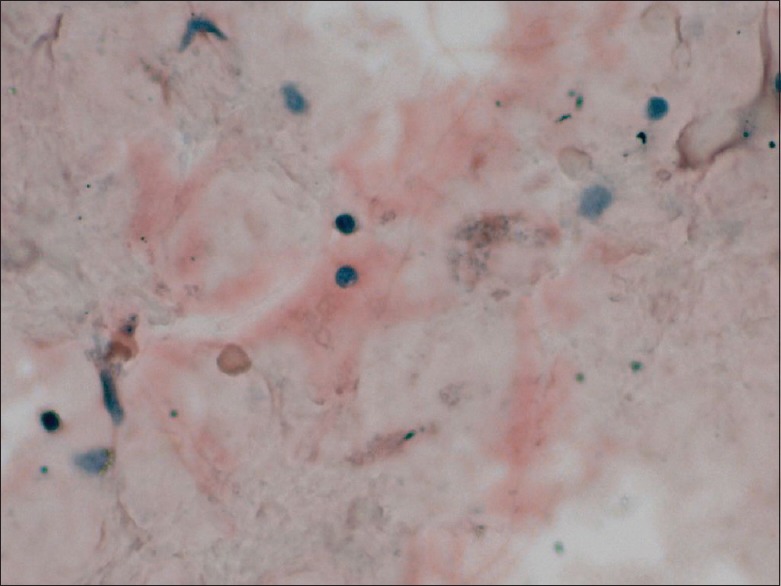
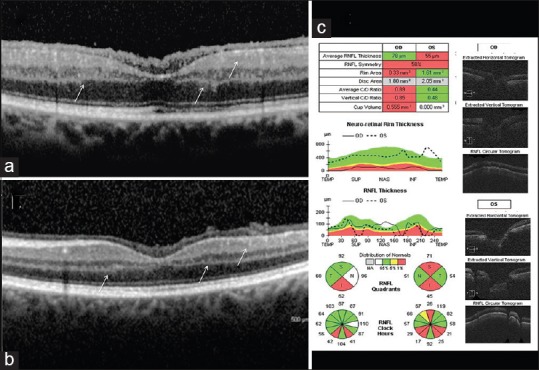
Pathological examination of material from a nonextensive pars plana vitrectomy (PPV) in the right eye provided a diagnosis of nonfamilial amyloidosis in a 68-year-old woman, who presented with bilateral glass wool-like vitreous opacities. Genetic testing revealed a Tyr114Cys mutation in the transthyretin gene. Six months after PPV, perimetry showed intense constriction with a temporal island and central scotoma in the right eye. An extensive PPV was performed in the left eye. Spectral domain optical coherence tomography evidenced bilateral epimacular amyloid deposits and unreported reflective spots within the inner retina. One year later, visual acuity had decreased to 20/400 in the left eye, with mild vitreous opacity, pale cupped optic disc and inferior altitudinal field defect. Bilateral diurnal intraocular pressure, transiently increased after PPV, never exceeded 16 mmHg with medication. Our patient presented optic nerve blood supply impairment, due to amyloidosis, which caused optic atrophy. Epiretinal and intraretinal deposit detection could aid in diagnosing patients with suspected amyloidosis.
Conflict of interest statement
Figures

References
-
- Kivelä T, Tarkkanen A, Frangione B, Ghiso J, Haltia M. Ocular amyloid deposition in familial amyloidosis, Finnish: An analysis of native and variant gelsolin in Meretoja's syndrome. Invest Ophthalmol Vis Sci. 1994;35:3759–69. - PubMed
-
- Haraoka K, Ando Y, Ando E, Sandgren O, Hirata A, Nakamura M, et al. Amyloid deposition in ocular tissues of patients with familial amyloidotic polyneuropathy (FAP) Amyloid. 2002;9:183–9. - PubMed
-
- Taban M, Piva A, See RF, Sadun AA, Quiros PA. Review: Orbital amyloidosis. Ophthal Plast Reconstr Surg. 2004;20:162–5. - PubMed
-
- Biswas J, Badrinath SS, Rao NA. Primary nonfamilial amyloidosis of the vitreous. A light microscopic and ultrastructural study. Retina. 1992;12:251–3. - PubMed
-
- Kimura A, Ando E, Fukushima M, Koga T, Hirata A, Arimura K, et al. Secondary glaucoma in patients with familial amyloidotic polyneuropathy. Arch Ophthalmol. 2003;121:351–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
