

Time-updated systolic blood pressure and the progression of chronic kidney disease: a cohort study
- PMID: 25686166
- PMCID: PMC4404622
- DOI: 10.7326/M14-0488
Time-updated systolic blood pressure and the progression of chronic kidney disease: a cohort study
Abstract
Background: Previous reports of the longitudinal association between achieved blood pressure (BP) and end-stage renal disease (ESRD) among patients with chronic kidney disease (CKD) have not incorporated time-updated BP with appropriate covariate adjustment.
Objective: To assess the association between baseline and time-updated systolic blood pressure (SBP) with CKD progression.
Design: Observational, prospective cohort study. (ClinicalTrials.gov: NCT00304148).
Setting: 7 U.S. clinical centers.
Patients: Patients in the Chronic Renal Insufficiency Cohort Study (n = 3708) followed for a median of 5.7 years (25th to 75th percentile, 4.6 to 6.7 years).
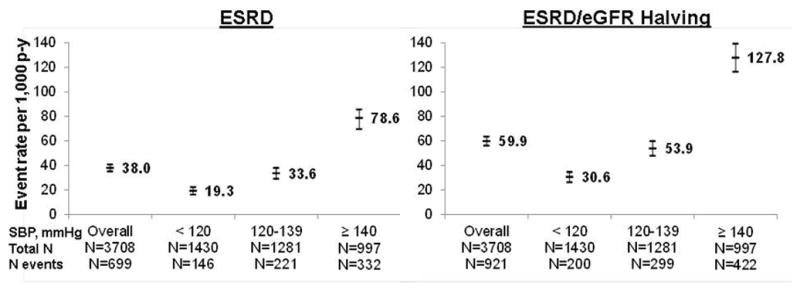
Measurements: The mean of 3 seated SBP measurements made up the visit-specific SBP. Time-updated SBP was the mean of that and all previous visits. Outcomes were ESRD and the composite end point of ESRD or halving of the estimated glomerular filtration rate. Analyses investigating baseline and time-updated SBP used Cox proportional hazards models and marginal structural models, respectively.
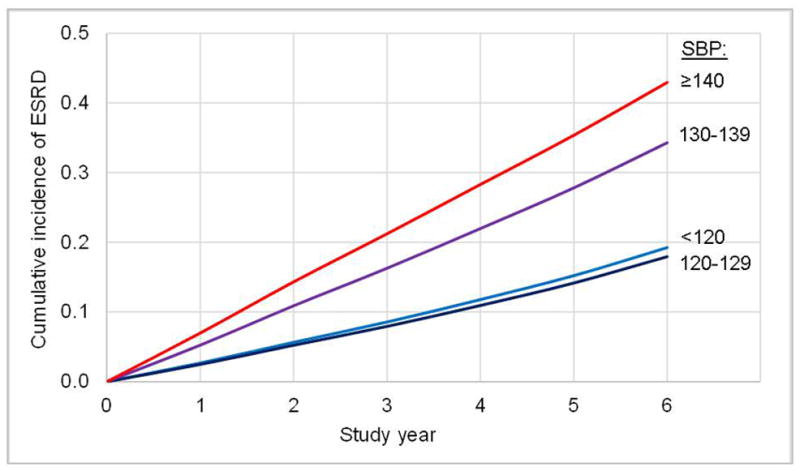
Results: Systolic blood pressure was 130 mm Hg or greater at all visits in 19.2% of patients. The hazard ratio for ESRD among patients with SBP of 130 to 139 mm Hg, compared with SBP less than 120 mm Hg, was 1.46 (95% CI, 1.13 to 1.88) using only baseline data and 2.37 (CI, 1.48 to 3.80) using time-updated data. Among patients with SBP of 140 mm Hg or greater, corresponding hazard ratios were 1.46 (CI, 1.18 to 1.88) and 3.37 (CI, 2.26 to 5.03) for models using only baseline data and those using time-updated data, respectively.
Limitation: Blood pressure was measured once annually, and the cohort was not a random sample.
Conclusion: Time-updated SBP greater than 130 mm Hg was more strongly associated with CKD progression than analyses based on baseline SBP.
Primary funding source: National Institute of Diabetes and Digestive and Kidney Diseases.
Conflict of interest statement
Dr. Chertow serves on the Board of Directors for Satellite Healthcare and PuraCath. He has received research support from Amgen, Keryx and Reata. He has served as an advisor to Allocure, Amgen, Ardelyx, Astra Zeneca, Gilead, Hemodialysis Plus, Keryx and Thrasos.
Dr. Townsend receives grant support from NIH, is a consultant for Janssen, Merck, GSK, Novartis, receives royalties from UpToDate, Jones & Bartlett, and has received honoraria or travel stipends from the American Society of Nephrology, American Society of Hypertension, and National Kidney Foundation.
Dr. Steigerwalt receives grant support from Medtronic, is a consultant for ATCOR, and has received honoraria from Takeda.
The remaining authors have no relevant conflicts to disclose.
Figures
References
-
- United States Renal Data System (USRDS) USRDS 2013 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2013. [Accessed last on June 17, 2014]. http://www.usrds.org/2013/pdf/v1_ch2_13.pdf.
-
- Klag MJ, Whelton PK, Randall BL, et al. Blood pressure and end-stage renal disease in men. N Engl J Med. 1996;334:13–18. - PubMed
-
- Tozawa M, Iseki K, Iseki C, Kinjo K, Ikemiya Y, Takishita S. Blood pressure predicts risk of developing end-stage renal disease in men and women. Hypertension. 2003;41:1341–1345. - PubMed
-
- Klahr S, Levey AS, Beck GJ, et al. The effects of dietary protein restriction and blood-pressure control on the progression of chronic renal disease. Modification of Diet in Renal Disease Study Group. N Engl J Med. 1994;330:877–884. - PubMed
-
- Wuhl E, Trivelli A, Picca S, et al. Strict blood-pressure control and progression of renal failure in children. N Engl J Med. 2009;361:1639–1650. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- K24 DK002651/DK/NIDDK NIH HHS/United States
- K24DK002651/DK/NIDDK NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- UL1RR-024131/RR/NCRR NIH HHS/United States
- U01DK060980/DK/NIDDK NIH HHS/United States
- P30GM103337/GM/NIGMS NIH HHS/United States
- U01DK061028/DK/NIDDK NIH HHS/United States
- K01DK092353/DK/NIDDK NIH HHS/United States
- U01DK060902/DK/NIDDK NIH HHS/United States
- M01-RR-16500/RR/NCRR NIH HHS/United States
- UL1 RR029879/RR/NCRR NIH HHS/United States
- U01 DK061028/DK/NIDDK NIH HHS/United States
- UL1 TR000433/TR/NCATS NIH HHS/United States
- R01 DK072231/DK/NIDDK NIH HHS/United States
- U01DK060963/DK/NIDDK NIH HHS/United States
- U01 DK060984/DK/NIDDK NIH HHS/United States
- U01 DK061021/DK/NIDDK NIH HHS/United States
- U01DK061022/DK/NIDDK NIH HHS/United States
- K01 DK092353/DK/NIDDK NIH HHS/United States
- P30 GM103337/GM/NIGMS NIH HHS/United States
- U01 DK060980/DK/NIDDK NIH HHS/United States
- UL1TR000433/TR/NCATS NIH HHS/United States
- U01 DK060963/DK/NIDDK NIH HHS/United States
- UL1 TR-000424/TR/NCATS NIH HHS/United States
- U01 DK061022/DK/NIDDK NIH HHS/United States
- U01DK061021/DK/NIDDK NIH HHS/United States
- U01DK060984/DK/NIDDK NIH HHS/United States
- UL1RR029879/RR/NCRR NIH HHS/United States
- U01DK060990/DK/NIDDK NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- UL1TR000003/TR/NCATS NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- M01 RR016500/RR/NCRR NIH HHS/United States
- U01 DK060902/DK/NIDDK NIH HHS/United States
- U01 DK060990/DK/NIDDK NIH HHS/United States
- UL1TR000439/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical