

An analysis of calibration and discrimination among multiple cardiovascular risk scores in a modern multiethnic cohort
- PMID: 25686167
- PMCID: PMC4414494
- DOI: 10.7326/M14-1281
An analysis of calibration and discrimination among multiple cardiovascular risk scores in a modern multiethnic cohort
Abstract
Background: Accurate risk assessment of atherosclerotic cardiovascular disease (ASCVD) is essential to effectively balance the risks and benefits of therapy for primary prevention.
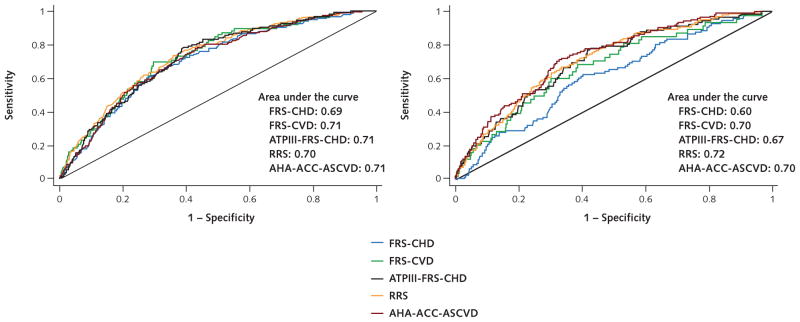
Objective: To compare the calibration and discrimination of the new American Heart Association (AHA) and American College of Cardiology (ACC) ASCVD risk score with alternative risk scores and to explore preventive therapy as a cause of the reported risk overestimation using the AHA-ACC-ASCVD score.
Design: Prospective epidemiologic study of ASCVD.
Setting: MESA (Multi-Ethnic Study of Atherosclerosis), a community-based, sex-balanced, multiethnic cohort.
Patients: 4227 MESA participants aged 50 to 74 years and without diabetes at baseline.
Measurements: Observed and expected events for the AHA-ACC-ASCVD score were compared with 4 commonly used risk scores-and their respective end points-in MESA after a 10.2-year follow-up.
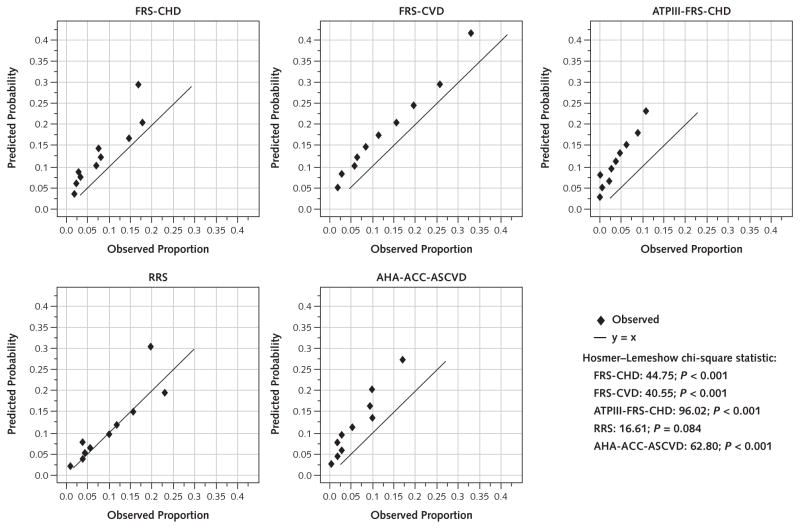
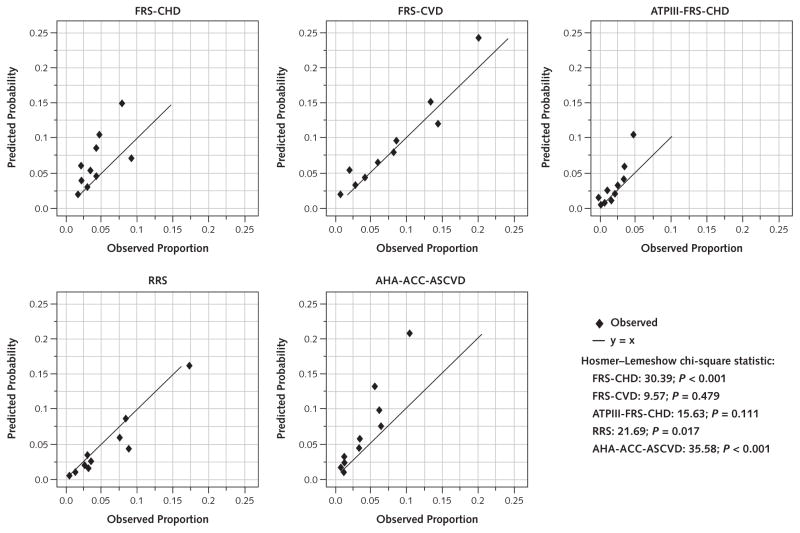
Results: The new AHA-ACC-ASCVD and 3 older Framingham-based risk scores overestimated cardiovascular events by 37% to 154% in men and 8% to 67% in women. Overestimation was noted throughout the continuum of risk. In contrast, the Reynolds Risk Score overestimated risk by 9% in men but underestimated risk by 21% in women. Aspirin, lipid-lowering or antihypertensive therapy, and interim revascularization did not explain the overestimation.
Limitation: Comparability of MESA with target populations for primary prevention and possibility of missed events in MESA.
Conclusion: Of the 5 risk scores, 4, including the new AHA-ACC-ASCVD score, showed overestimation of risk (25% to 115%) in a modern, multiethnic cohort without baseline clinical ASCVD. If validated, overestimation of ASCVD risk may have substantial implications for individual patients and the health care system.
Primary funding source: National Heart, Lung, and Blood Institute.
Figures
Comment in
-
Comparing cardiovascular risk prediction scores.Ann Intern Med. 2015 Feb 17;162(4):313-4. doi: 10.7326/M14-2820. Ann Intern Med. 2015. PMID: 25686171 No abstract available.
-
Calibration and Discrimination Among Multiple Cardiovascular Risk Scores in a Modern Multiethnic Cohort.Ann Intern Med. 2015 Jul 7;163(1):68. doi: 10.7326/L15-5105. Ann Intern Med. 2015. PMID: 26148286 No abstract available.
-
Calibration and Discrimination Among Multiple Cardiovascular Risk Scores in a Modern Multiethnic Cohort.Ann Intern Med. 2015 Jul 7;163(1):68-9. doi: 10.7326/L15-5105-2. Ann Intern Med. 2015. PMID: 26148287 No abstract available.
-
ACP Journal Club. In adults without CV disease, most prediction scores overestimated risk for atherosclerotic CV events.Ann Intern Med. 2015 Jul 21;163(2):JC13. doi: 10.7326/ACPJC-2015-163-2-013. Ann Intern Med. 2015. PMID: 26192581 No abstract available.
References
-
- Fletcher B, Berra K, Ades P, Braun LT, Burke LE, Durstine JL, et al. Council on Cardiovascular Nursing. Managing abnormal blood lipids: a collaborative approach. Circulation. 2005;112:3184–209. - PubMed
-
- Goldstein LB, Bushnell CD, Adams RJ, Appel LJ, Braun LT, Chaturvedi S, et al. American Heart Association Stroke Council. . Guidelines for the primary prevention of stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011;42:517–84. doi: 10.1161/STR.0b013e3181fcb238. - DOI - PubMed
-
- Mosca L, Benjamin EJ, Berra K, Bezanson JL, Dolor RJ, Lloyd-Jones DM, et al. Effectiveness-based guidelines for the prevention of cardiovascular disease in women—2011 update: a guideline from the American Heart Association. Circulation. 2011;123:1243–62. doi: 10.1161/CIR.0b013e31820faaf8. - DOI - PMC - PubMed
-
- Wilson PW, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coronary heart disease using risk factor categories. Circulation. 1998;97:1837–47. - PubMed
-
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:3143–421. - PubMed