

Integrated primary care for patients with mental and physical multimorbidity: cluster randomised controlled trial of collaborative care for patients with depression comorbid with diabetes or cardiovascular disease
- PMID: 25687344
- PMCID: PMC4353275
- DOI: 10.1136/bmj.h638
Integrated primary care for patients with mental and physical multimorbidity: cluster randomised controlled trial of collaborative care for patients with depression comorbid with diabetes or cardiovascular disease
Abstract
Objective: To test the effectiveness of an integrated collaborative care model for people with depression and long term physical conditions.
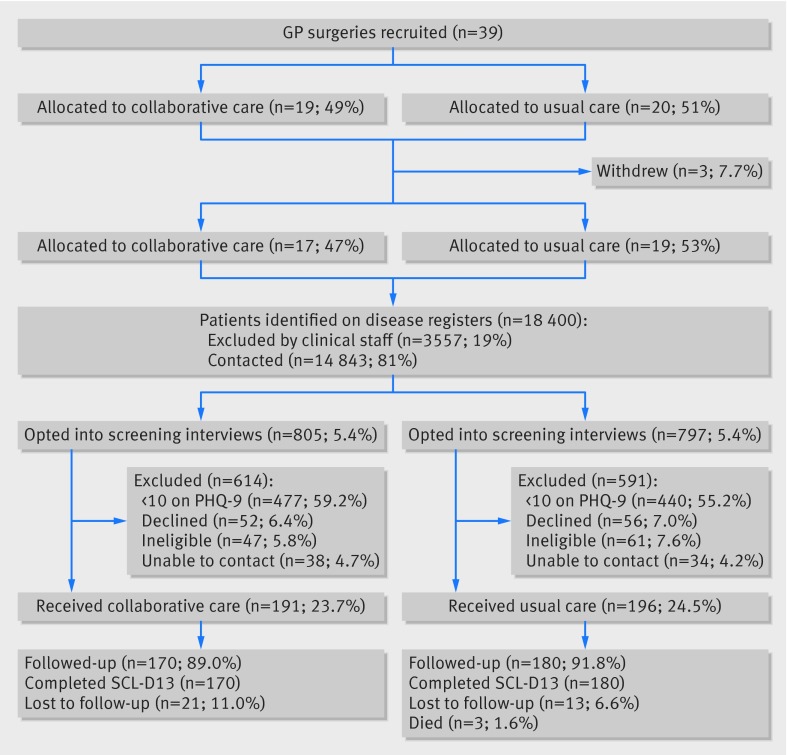
Design: Cluster randomised controlled trial.
Setting: 36 general practices in the north west of England.
Participants: 387 patients with a record of diabetes or heart disease, or both, who had depressive symptoms (≥ 10 on patient health questionaire-9 (PHQ-9)) for at least two weeks. Mean age was 58.5 (SD 11.7). Participants reported a mean of 6.2 (SD 3.0) long term conditions other than diabetes or heart disease; 240 (62%) were men; 360 (90%) completed the trial.
Interventions: Collaborative care included patient preference for behavioural activation, cognitive restructuring, graded exposure, and/or lifestyle advice, management of drug treatment, and prevention of relapse. Up to eight sessions of psychological treatment were delivered by specially trained psychological wellbeing practitioners employed by Improving Access to Psychological Therapy services in the English National Health Service; integration of care was enhanced by two treatment sessions delivered jointly with the practice nurse. Usual care was standard clinical practice provided by general practitioners and practice nurses.
Main outcome measures: The primary outcome was reduction in symptoms of depression on the self reported symptom checklist-13 depression scale (SCL-D13) at four months after baseline assessment. Secondary outcomes included anxiety symptoms (generalised anxiety disorder 7), self management (health education impact questionnaire), disability (Sheehan disability scale), and global quality of life (WHOQOL-BREF).
Results: 19 general practices were randomised to collaborative care and 20 to usual care; three practices withdrew from the trial before patients were recruited. 191 patients were recruited from practices allocated to collaborative care, and 196 from practices allocated to usual care. After adjustment for baseline depression score, mean depressive scores were 0.23 SCL-D13 points lower (95% confidence interval -0.41 to -0.05) in the collaborative care arm, equal to an adjusted standardised effect size of 0.30. Patients in the intervention arm also reported being better self managers, rated their care as more patient centred, and were more satisfied with their care. There were no significant differences between groups in quality of life, disease specific quality of life, self efficacy, disability, and social support.
Conclusions: Collaborative care that incorporates brief low intensity psychological therapy delivered in partnership with practice nurses in primary care can reduce depression and improve self management of chronic disease in people with mental and physical multimorbidity. The size of the treatment effects were modest and were less than the prespecified effect but were achieved in a trial run in routine settings with a deprived population with high levels of mental and physical multimorbidity.
Trial registration: ISRCTN80309252.
© Coventry et al 2015.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Designing care for people with mixed mental and physical multimorbidity.BMJ. 2015 Feb 17;350:h712. doi: 10.1136/bmj.h712. BMJ. 2015. PMID: 25690275 No abstract available.
-
Author's reply to Sharpe.BMJ. 2015 Mar 10;350:h1288. doi: 10.1136/bmj.h1288. BMJ. 2015. PMID: 25757466 No abstract available.
-
Not all forms of collaborative care are the same.BMJ. 2015 Mar 10;350:h1287. doi: 10.1136/bmj.h1287. BMJ. 2015. PMID: 25758921 No abstract available.
-
A collaborative care approach delivering treatment to patients with depression comorbid with diabetes or cardiovascular disease achieves significant but small improvements over usual care in depression and patient satisfaction.Evid Based Ment Health. 2015 Nov;18(4):122. doi: 10.1136/eb-2015-102099. Epub 2015 Sep 21. Evid Based Ment Health. 2015. PMID: 26392401 Free PMC article. No abstract available.
References
-
- Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet 2012;380:37-43. - PubMed
-
- Moussavi S, Chatterji S, Verdes E, Tandon A, Patel V, Ustun B. Depression, chronic diseases, and decrements in health: results from the World Health Surveys. Lancet 2007;370:851-8. - PubMed
-
- Naylor C, Parsonage M, McDaid D, Knapp M, Fossey M, Galea A. Long-term conditions and mental health. The cost of co-morbidities. King’s Fund and Centre for Mental Health, 2012.
-
- Carney RM, Freedland KE, Sheps DS. Depression is a risk factor for mortality in coronary heart disease. Psychosom Med 2004;66:799-801. - PubMed
-
- Hjerl K, Andersen EW, Keiding N, Mouridsen HT, Mortensen PB, Jorgensen T. Depression as a prognostic factor for breast cancer mortality. Psychosomatics 2003;44:24-30. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous