

Predicting pulmonary hypertension with standard computed tomography pulmonary angiography
- PMID: 25687575
- PMCID: PMC4428842
- DOI: 10.1007/s10554-015-0618-x
Predicting pulmonary hypertension with standard computed tomography pulmonary angiography
Abstract
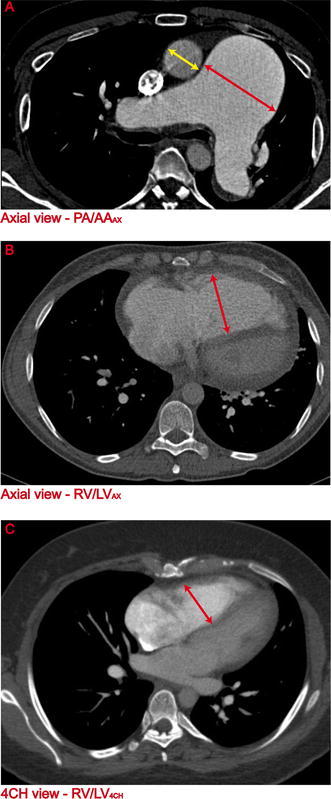
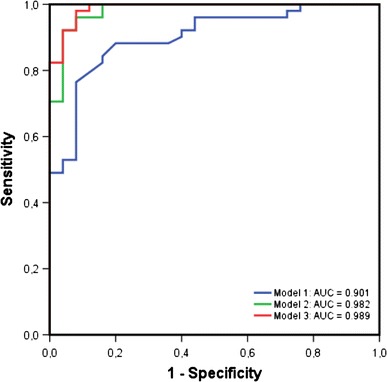
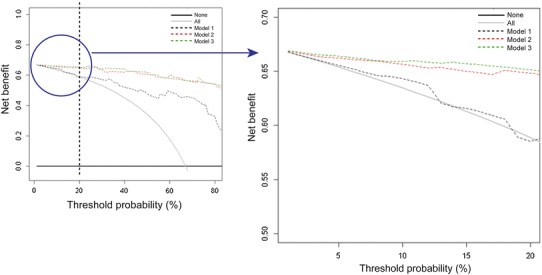
The most common feature of pulmonary hypertension (PH) on computed tomography pulmonary angiography (CTPA) is an increased diameter-ratio of the pulmonary artery to the ascending aorta (PA/AAAX). The aim of this study was to investigate whether combining PA/AAAX measurements with ventricular measurements improves the predictive value of CTPA for precapillary PH. Three predicting models were analysed using baseline CTPA scans of 51 treatment naïve precapillary PH patients and 25 non-PH controls: model 1: PA/AAAX only; model 2: PA/AAAX combined with the ratio of the right ventricular and left ventricular diameter measured on the axial view (RV/LVAX); model 3: PA/AAAX combined with the RV/LV-ratio measured on a four chamber view (RV/LV4CH). Prediction models were compared using multivariable binary logistic regression, ROC analyses and decision curve analyses (DCA). Multivariable binary logistic regression showed an improvement of the predictive value of model 2 (-2LL = 26.48) and 3 (-2LL = 21.03) compared to model 1 (-2LL = 21.03). ROC analyses showed significantly higher AUCs of model 2 and 3 compared to model 1 (p = 0.011 and p = 0.007, respectively). DCA showed an increased clinical benefit of model 2 and 3 compared to model 1. The predictive value of model 2 and 3 were almost equal. We found an optimal cut-off value for the RV/LV-ratio for predicting precapillary PH of RV/LV ≥ 1.20. The predictive value of CTPA for precapillary PH improves when ventricular and pulmonary artery measurements are combined. A PA/AAAX ≥ 1 or a RV/LVAX ≥ 1.20 needs further diagnostic evaluation to rule out or confirm the diagnosis.
Figures
Similar articles
-
A four-tier classification system of pulmonary artery metrics on computed tomography for the diagnosis and prognosis of pulmonary hypertension.J Cardiovasc Comput Tomogr. 2018 Jan-Feb;12(1):60-66. doi: 10.1016/j.jcct.2017.12.001. Epub 2017 Dec 6. J Cardiovasc Comput Tomogr. 2018. PMID: 29254655 Free PMC article.
-
Left Atrial Area and Right Ventricle Dimensions in Non-gated Axial Chest CT can Differentiate Pulmonary Hypertension Due to Left Heart Disease from Other Causes.J Cardiovasc Comput Tomogr. 2016 May-Jun;10(3):246-50. doi: 10.1016/j.jcct.2016.01.014. Epub 2016 Jan 30. J Cardiovasc Comput Tomogr. 2016. PMID: 26869368
-
Utility of Automated Cardiac Chamber Volumetry by Nongated CT Pulmonary Angiography for Detection of Pulmonary Hypertension Using the 2018 Updated Hemodynamic Definition.AJR Am J Roentgenol. 2022 Jul;219(1):66-75. doi: 10.2214/AJR.21.27147. Epub 2022 Jan 26. AJR Am J Roentgenol. 2022. PMID: 35080457
-
Chronic thromboembolic pulmonary hypertension (CTEPH) - potential role of multidetector-row CT (MD-CT) and MR imaging in the diagnosis and differential diagnosis of the disease.Rofo. 2014 Aug;186(8):751-61. doi: 10.1055/s-0034-1366425. Epub 2014 Apr 22. Rofo. 2014. PMID: 24756429 Review.
-
Advanced imaging in pulmonary hypertension: emerging techniques and applications.Int J Cardiovasc Imaging. 2019 Aug;35(8):1407-1420. doi: 10.1007/s10554-018-1448-4. Epub 2018 Aug 30. Int J Cardiovasc Imaging. 2019. PMID: 30168011 Review.
Cited by
-
The Role of Imaging in Pulmonary Vascular Disease: The Clinician's Perspective.Radiol Clin North Am. 2025 Mar;63(2):305-313. doi: 10.1016/j.rcl.2024.07.008. Epub 2024 Nov 29. Radiol Clin North Am. 2025. PMID: 39863382 Review.
-
Fully automatic cardiac four chamber and great vessel segmentation on CT pulmonary angiography using deep learning.Front Cardiovasc Med. 2022 Sep 26;9:983859. doi: 10.3389/fcvm.2022.983859. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36225963 Free PMC article.
-
CT imaging biomarkers to predict severity and prognosis of pulmonary hypertension.PLoS One. 2025 Feb 12;20(2):e0313235. doi: 10.1371/journal.pone.0313235. eCollection 2025. PLoS One. 2025. PMID: 39937766 Free PMC article.
-
Diagnostic accuracy of CT pulmonary angiography in suspected pulmonary hypertension.Eur Radiol. 2020 Sep;30(9):4918-4929. doi: 10.1007/s00330-020-06846-1. Epub 2020 Apr 27. Eur Radiol. 2020. PMID: 32342182 Free PMC article.
-
Unenhanced computed tomography as a diagnostic tool in suspected pulmonary hypertension: a retrospective cross-sectional pilot study.Wellcome Open Res. 2024 Jul 26;6:249. doi: 10.12688/wellcomeopenres.16853.2. eCollection 2021. Wellcome Open Res. 2024. PMID: 39113847 Free PMC article.
References
-
- Galie N, Hoeper MM, Humbert M, Torbicki A, Vachiery JL, Barbera JA, Beghetti M, Corris P, Gaine S, Gibbs JS, Gomez-Sanchez MA, Jondeau G, Klepetko W, Opitz C, Peacock A, Rubin L, Zellweger M, Simonneau G. Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J. 2009;34:1219–12163. doi: 10.1183/09031936.00139009. - DOI - PubMed
-
- Ling Y, Johnson MK, Kiely DG, Condliffe R, Elliot CA, Gibbs JS, Howard LS, Pepke-Zaba J, Sheares KK, Corris PA, Fisher AJ, Lordan JL, Gaine S, Coghlan JG, Wort SJ, Gatzoulis MA, Peacock AJ. Changing demographics, epidemiology, and survival of incident pulmonary arterial hypertension: results from the pulmonary hypertension registry of the United Kingdom and Ireland. Am J Respir Crit Care Med. 2012;186:790–796. doi: 10.1164/rccm.201203-0383OC. - DOI - PubMed
-
- Badesch DB, Raskob GE, Elliott CG, Krichman AM, Farber HW, Frost AE, Barst RJ, Benza RL, Liou TG, Turner M, Giles S, Feldkircher K, Miller DP, McGoon MD. Pulmonary arterial hypertension: baseline characteristics from the REVEAL Registry. Chest. 2010;137:376–387. doi: 10.1378/chest.09-1140. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
