

Cutaneous leishmaniasis: recent developments in diagnosis and management
- PMID: 25687688
- PMCID: PMC4363483
- DOI: 10.1007/s40257-015-0114-z
Cutaneous leishmaniasis: recent developments in diagnosis and management
Abstract
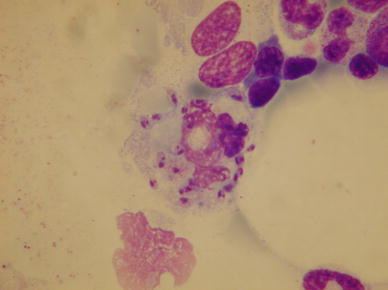
This review focuses on recent developments in the diagnosis, treatment, management, and strategies for the prevention and control of cutaneous leishmaniasis (CL) caused by both Old and New World Leishmania species. CL is caused by the vector-borne protozoan parasite Leishmania and is transmitted via infected female sandflies. The disease is endemic in more than 98 countries and an estimated 350 million people are at risk. The overall prevalence is 12 million cases and the annual incidence is 2-2.5 million. The World Health Organization considers CL a severely neglected disease and a category 1 emerging and uncontrolled disease. The management of CL differs from region to region and is primarily based on local experience-based evidence. Most CL patients can be treated with topical treatments, but some Leishmania species can cause mucocutaneous involvement requiring a systemic therapeutic approach. Moreover, Leishmania species can vary in their sensitivity to available therapeutic options. This makes species determination critical for the choice of treatment and the clinical outcome of CL. Identification of the infecting parasite used to be laborious, but now the Leishmania species can be identified relatively easy with new DNA techniques that enable a more rational therapy choice. Current treatment guidelines for CL are based on poorly designed and reported trials. There is a lack of evidence for potentially beneficial treatments, a desperate need for large well-conducted studies, and standardization of future trials. Moreover, intensified research programs to improve vector control, diagnostics, and the therapeutic arsenal to contain further incidence and morbidity are needed.
Figures




References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
