

Comparing language outcomes in monolingual and bilingual stroke patients
- PMID: 25688076
- PMCID: PMC5014078
- DOI: 10.1093/brain/awv020
Comparing language outcomes in monolingual and bilingual stroke patients
Erratum in
-
Corrigendum.Brain. 2017 Aug 1;140(8):e54. doi: 10.1093/brain/awx079. Brain. 2017. PMID: 28379499 Free PMC article. No abstract available.
Abstract
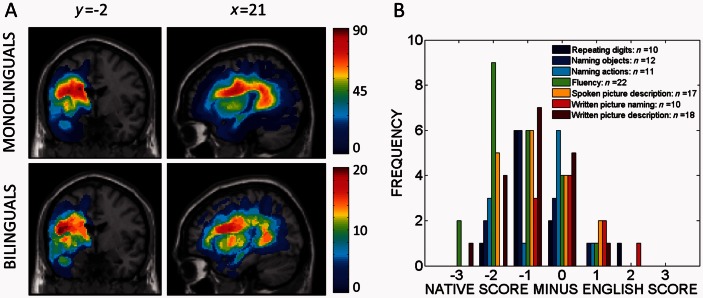
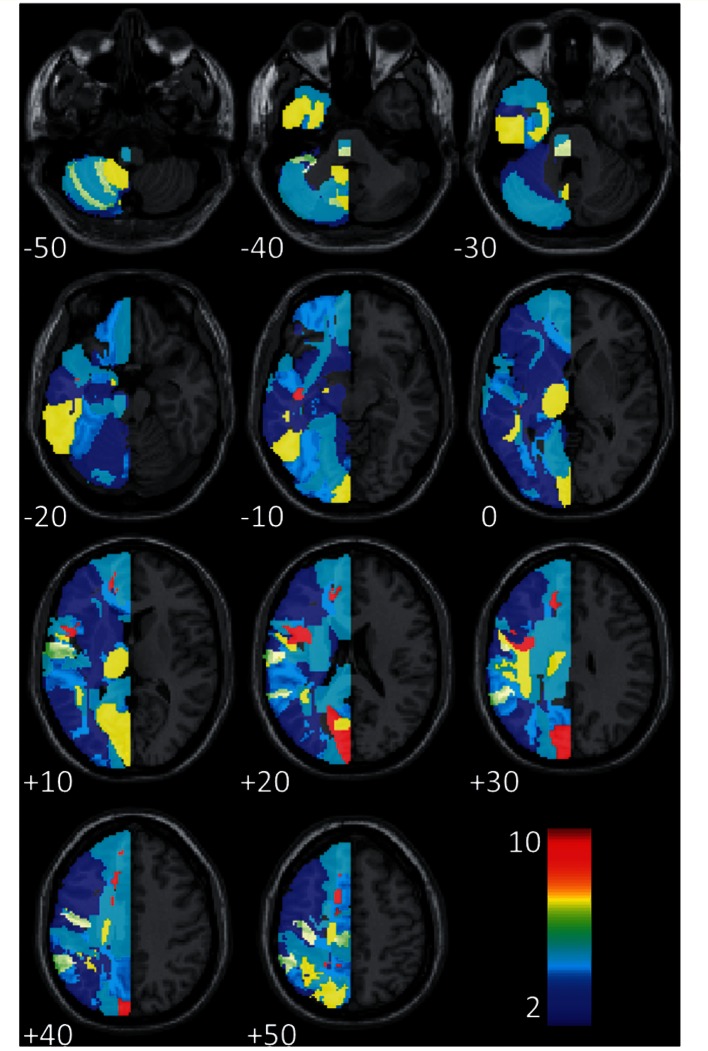
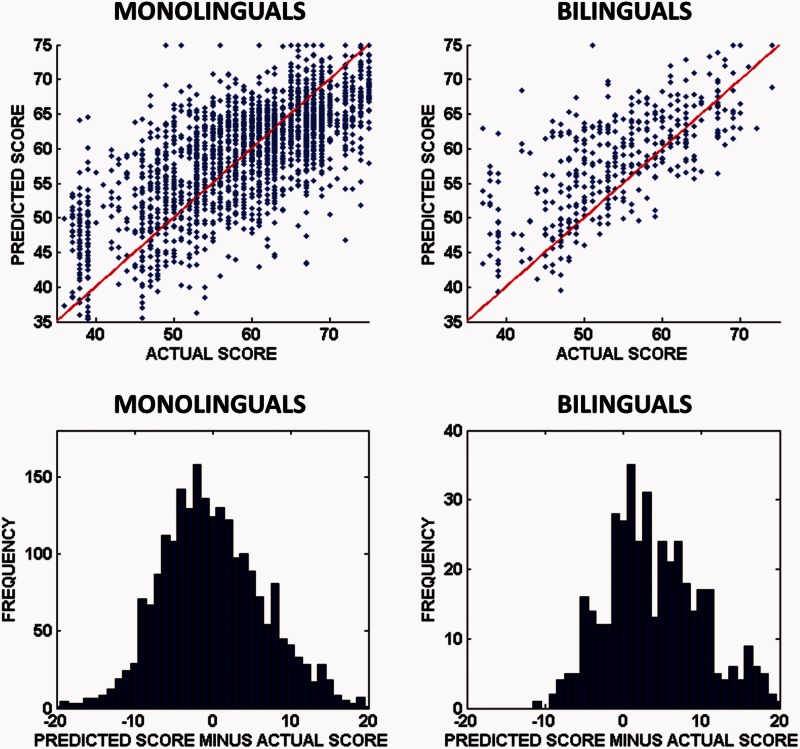
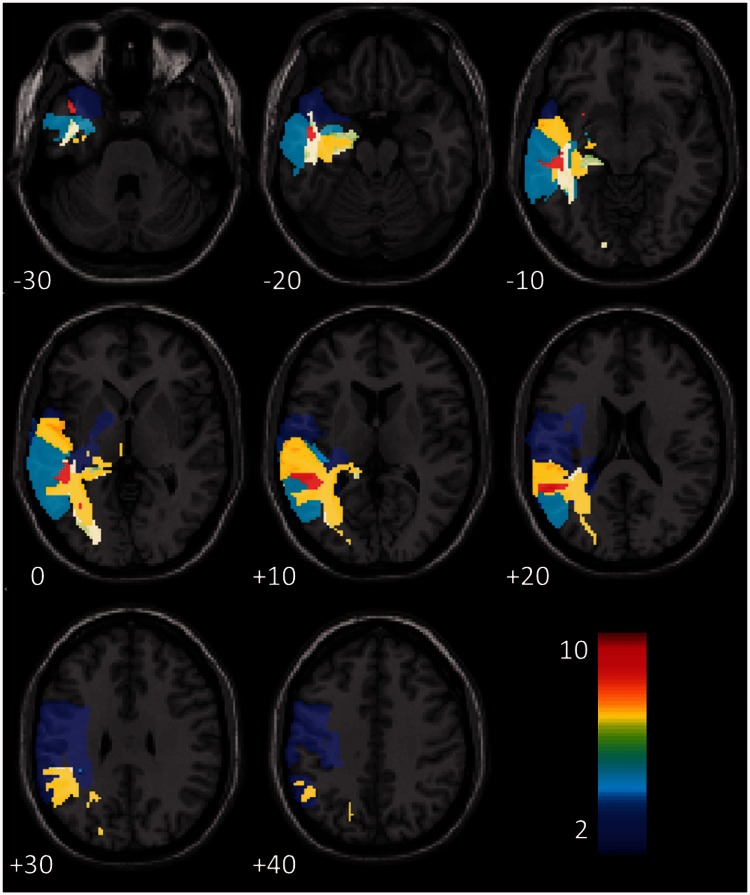
Post-stroke prognoses are usually inductive, generalizing trends learned from one group of patients, whose outcomes are known, to make predictions for new patients. Research into the recovery of language function is almost exclusively focused on monolingual stroke patients, but bilingualism is the norm in many parts of the world. If bilingual language recruits qualitatively different networks in the brain, prognostic models developed for monolinguals might not generalize well to bilingual stroke patients. Here, we sought to establish how applicable post-stroke prognostic models, trained with monolingual patient data, are to bilingual stroke patients who had been ordinarily resident in the UK for many years. We used an algorithm to extract binary lesion images for each stroke patient, and assessed their language with a standard tool. We used feature selection and cross-validation to find 'good' prognostic models for each of 22 different language skills, using monolingual data only (174 patients; 112 males and 62 females; age at stroke: mean = 53.0 years, standard deviation = 12.2 years, range = 17.2-80.1 years; time post-stroke: mean = 55.6 months, standard deviation = 62.6 months, range = 3.1-431.9 months), then made predictions for both monolinguals and bilinguals (33 patients; 18 males and 15 females; age at stroke: mean = 49.0 years, standard deviation = 13.2 years, range = 23.1-77.0 years; time post-stroke: mean = 49.2 months, standard deviation = 55.8 months, range = 3.9-219.9 months) separately, after training with monolingual data only. We measured group differences by comparing prediction error distributions, and used a Bayesian test to search for group differences in terms of lesion-deficit associations in the brain. Our models distinguish better outcomes from worse outcomes equally well within each group, but tended to be over-optimistic when predicting bilingual language outcomes: our bilingual patients tended to have poorer language skills than expected, based on trends learned from monolingual data alone, and this was significant (P < 0.05, corrected for multiple comparisons) in 13/22 language tasks. Both patient groups appeared to be sensitive to damage in the same sets of regions, though the bilinguals were more sensitive than the monolinguals. media-1vid1 10.1093/brain/awv020_video_abstract awv020_video_abstract.
Keywords: aphasia; bilingualism; language; prognosis; stroke.
© The Author (2015). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
References
-
- Abutalebi J. Neural aspects of second language representation and language control. Acta Psychol. 2008;128:466–78. - PubMed
-
- Abutalebi J, Green D. Bilingual language production: the neurocognition of language representation and control. J Neurolinguistics. 2007;20:242–75.
-
- Abutalebi J, Rosa PA, Tettamanti M, Green DW, Cappa SF. Bilingual aphasia and language control: a follow-up fMRI and intrinsic connectivity study. Brain Lang. 2009;109:141–56. - PubMed
-
- Alladi S, Bak TH, Duggirala V, Surampudi B, Shailaja M, Shukla AK, et al. Bilingualism delays age at onset of dementia, independent of education and immigration status. Neurology. 2013;81:1938–44. - PubMed
-
- Ashburner J, Friston KJ. Unified segmentation. NeuroImage. 2005;26:839–51. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
