

Safety of ventricular tachycardia ablation in clinical practice: findings from 9699 hospital discharge records
- PMID: 25688143
- PMCID: PMC9893573
- DOI: 10.1161/CIRCEP.114.002336
Safety of ventricular tachycardia ablation in clinical practice: findings from 9699 hospital discharge records
Abstract
Background: Outcomes of ventricular tachycardia (VT) ablation have been described in clinical trials and single-center studies. We assessed the safety of VT ablation in clinical practice.
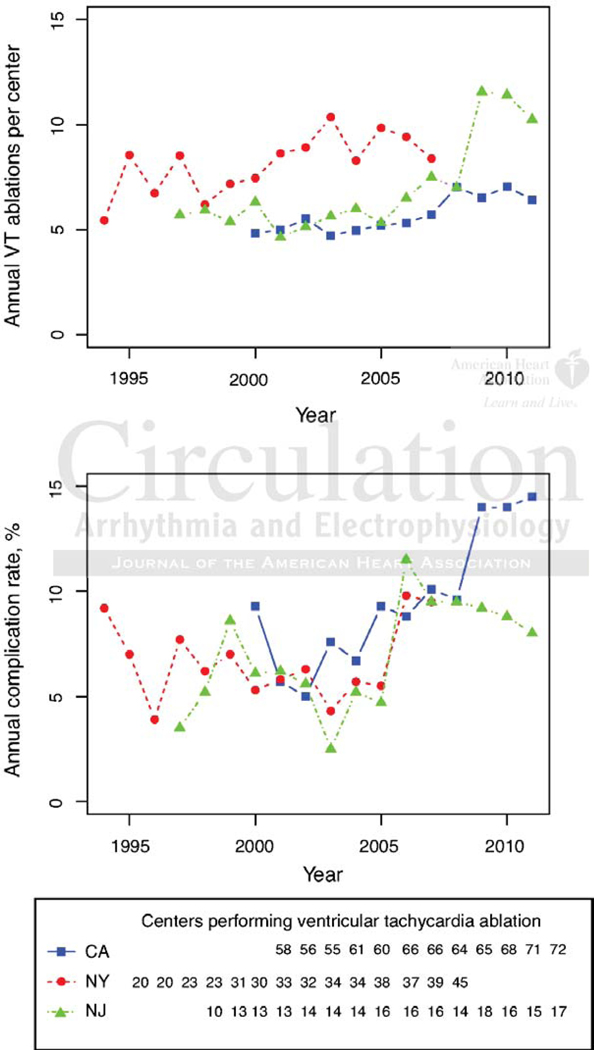
Methods and results: Using administrative hospitalization data between 1994 and 2011, we identified hospitalizations with primary diagnosis of VT (International Classification of Diseases-9 Clinical Modification code: 427.1) and cardiac ablation (International Classification of Diseases-9 Clinical Modification code: 37.34). We quantified in-hospital adverse events (AEs), including death, stroke, intracerebral hemorrhage, pericardial complications, hematoma or hemorrhage, blood transfusion, or cardiogenic shock. Secondary outcomes included major AEs (stroke, tamponade, or death) and death. Multivariable mixed effects models identified patient and hospital characteristics associated with AEs. Of 9699 hospitalizations with VT ablations (age, 56.5 ± 17.6; 60.1% men), AEs were reported in 825 (8.5%), major AEs in 295 (3.0%), and death in 110 (1.1%). Heart failure had the strongest association with death (odds ratio, 5.52; 95% confidence interval, 2.97-10.3) and major AE (odds ratio, 2.99; 95% confidence interval, 2.15-4.16). Anemia (odds ratio, 4.84; 95% confidence interval, 3.79-6.19) and unscheduled admission (odds ratio, 1.64; 95% confidence interval, 1.37-1.97) were associated with AEs. During the study period, incidence of AEs increased from 9.2% to 12.8% as did the burden of AE risk factors (0.034 patient/y; P < 0.001). Hospital volume > 25 cases/y was associated with fewer AEs compared with lower volume centers (6.4% versus 8.8%; P = 0.008).
Conclusions: VT ablation-associated AE rates in clinical practice are similar to those reported in the literature. Over time rates have increased as have the number of AE risk factors per patient. Ablations done electively and at hospitals with higher procedural volume are associated with lower incidence of AEs.
Keywords: catheter ablation; complication; tachycardia.
© 2015 American Heart Association, Inc.
Conflict of interest statement
Figures


References
-
- Palaniswamy C, Kolte D, Harikrishnan P, Khera S, Aronow WS, Mujib M, Mellana WM, Eugenio P, Lessner S, Ferrick A, Fonarow GC, Ahmed A, Cooper HA, Frishman WH, Panza JA, Iwai S. Catheter Ablation of Post-Infarction Ventricular Tachycardia: Ten-Year Trends in Utilization, In-Hospital Complications, and In-Hospital Mortality in the United States. Heart Rhythm. 2014;11:2056–2063. - PubMed
-
- de Loma-Osorio AF, Diaz-Infante E, Gallego AM. Spanish Catheter Ablation Registry. 12th Official Report of the Spanish Society of Cardiology Working Group on Electrophysiology and Arrhythmias (2012). Rev Esp Cardiol. 2013;66:983–992. - PubMed
-
- Calkins H, Kalbfleisch SJ, el-Atassi R, Langberg JJ, Morady F. Relation between efficacy of radiofrequency catheter ablation and site of origin of idiopathic ventricular tachycardia. Am J Cardiol. 1993;71:827–833. - PubMed
-
- Calkins H, Epstein A, Packer D, Arria AM, Hummel J, Gilligan DM, Trusso J, Carlso M, Luceri R, Kopelman H, Wilber D, Wharton JM, Stevenson W. Catheter ablation of ventricular tachycardia in patients with structural heart disease using cooled radiofrequency energy: results of a prospective multicenter study. Cooled RF Multi Center Investigators Group. J Am Coll Cadiol. 2000;35:1905–1914. - PubMed
-
- Joshi S, Wilber DJ. Ablation of idiopathic right ventricular outflow tract tachycardia: current perspectives. JCardiovasc Electrophysiol. 2005;16 Suppl 1:S52–S58. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
