

Review
doi: 10.1155/2015/543412.
Epub 2015 Jan 19.
Acute compartment syndrome in orthopedics: causes, diagnosis, and management
Affiliations
- PMID: 25688303
- PMCID: PMC4320895
- DOI: 10.1155/2015/543412
Item in Clipboard
Review
Acute compartment syndrome in orthopedics: causes, diagnosis, and management
Adv Orthop.
2015.
Abstract
Almost all orthopaedic surgeons come across acute compartment syndrome (ACS) in their clinical practice. Diagnosis of ACS mostly relies on clinical findings. If the diagnosis is missed and left untreated, it can lead to serious consequences which can endanger limb and life of the patient and also risk the clinician to face lawsuits. This review article highlights the characteristic features of ACS which will help an orthopaedic surgeon to understand the pathophysiology, natural history, high risk patients, diagnosis, and surgical management of the condition.
Figures
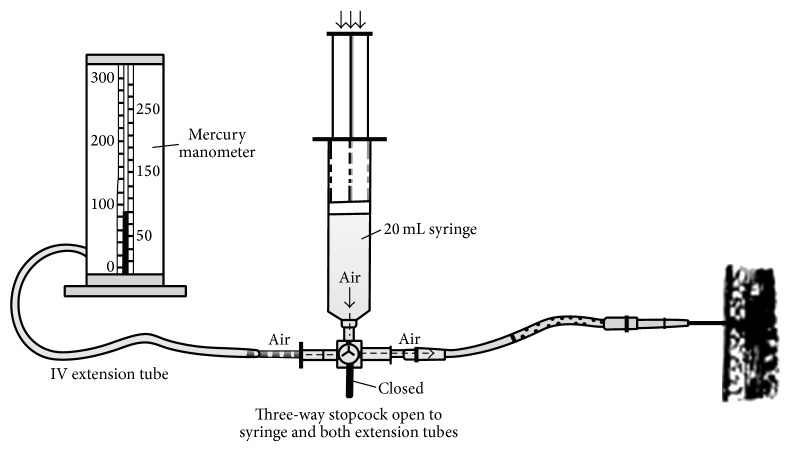
Manual setup for intracompartmental pressure measurement (Campbell Operative Orthopaedics, 11th Edition).

Stryker digital device.
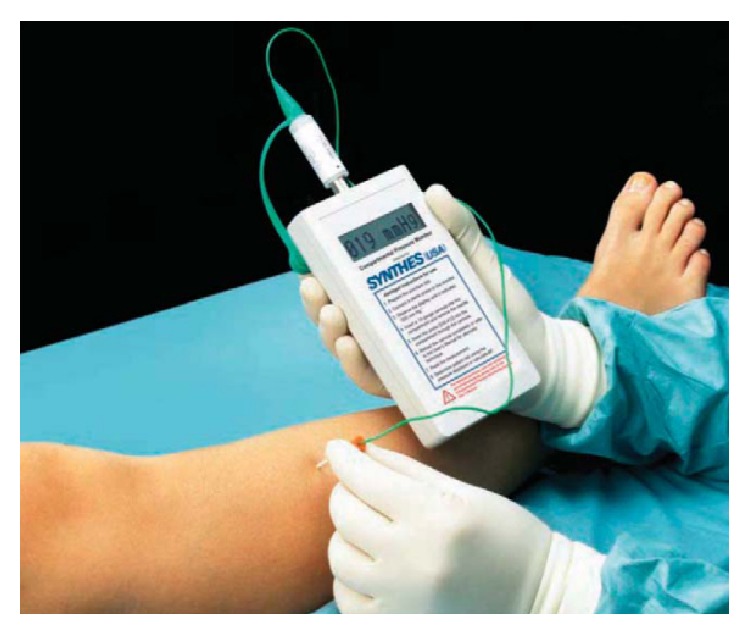
Synthes (West Chester, PA) hand-held compartment pressure monitor.
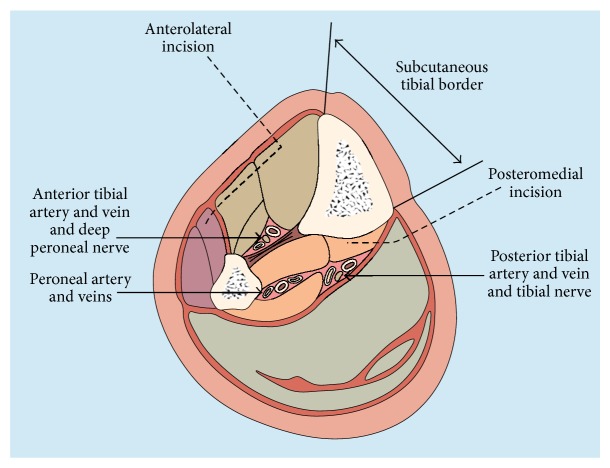
Cross section through leg showing site of fasciotomy incisions to decompress all four compartments [31].
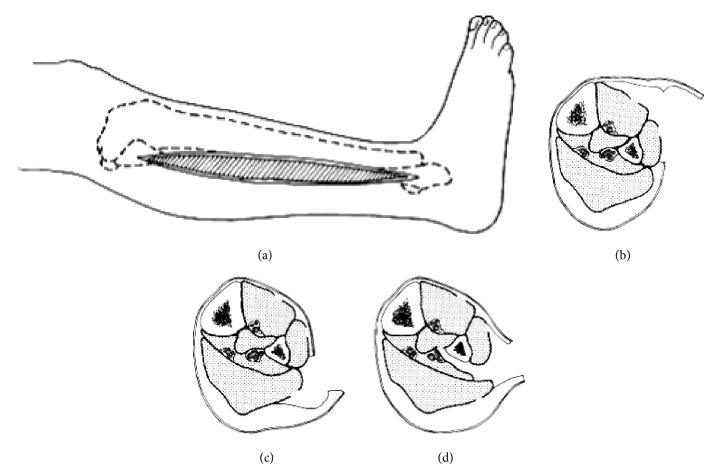
One-incision technique without fibulectomy. (a) Lateral skin incision from fibular neck 3 to 4 cm proximal to lateral malleolus. (b) Skin is undermined anteriorly, and fasciotomy of anterior and lateral compartments is performed. (c) Skin is undermined posteriorly, and fasciotomy of superficial posterior compartment is performed. (d) Interval between superficial posterior and lateral compartments is developed. Flexor hallucis longus muscle is dissected subperiosteally off fibula and retracted posteromedially. Fascial attachment of posterior tibial muscle to fibula is incised to decompress muscle (redrawn from [34]).

The volar S shaped incision including proximal palm to decompress carpal tunnel.
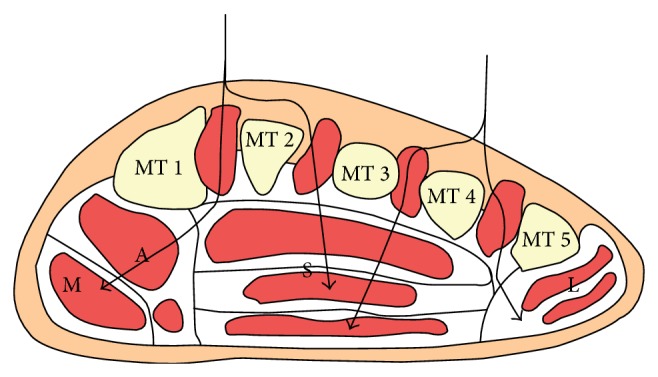
Anatomical section view of the forefoot. The dorsal approach uses one or two longitudinal incisions. It facilitates access to the interosseus and adductor compartments. MT = metatarsal; M = medial compartment; A = adductor compartment; S = superficial compartment; L = lateral compartment.

Dynamic wound closure using the vessel loop or shoelace technique.
References
-
- Volkmann R. Die ischaemischen Muskellähmungen und Kontrakturen. Zentralblatt für Chirurgie. 1881;8:801–803.
-
- Rorabeck C. H. The treatment of compartment syndromes of the leg. Journal of Bone and Joint Surgery. 1984;66(1):94–97. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
