

Frequency and prognostic significance of p16(INK4A) protein overexpression and transcriptionally active human papillomavirus infection in laryngeal squamous cell carcinoma
- PMID: 25688737
- PMCID: PMC4366899
- DOI: 10.1038/bjc.2015.59
Frequency and prognostic significance of p16(INK4A) protein overexpression and transcriptionally active human papillomavirus infection in laryngeal squamous cell carcinoma
Abstract
Background: Human papillomavirus (HPV) infection is a powerful prognostic biomarker in a subset of head and neck squamous cell carcinomas, specifically oropharyngeal cancers. However, the role of HPV in non-oropharyngeal sites, such as the larynx, remains unconfirmed.
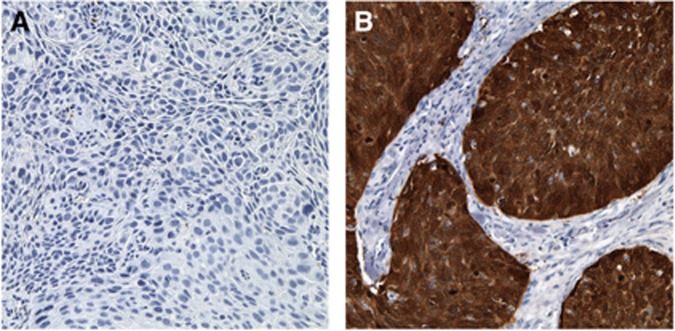
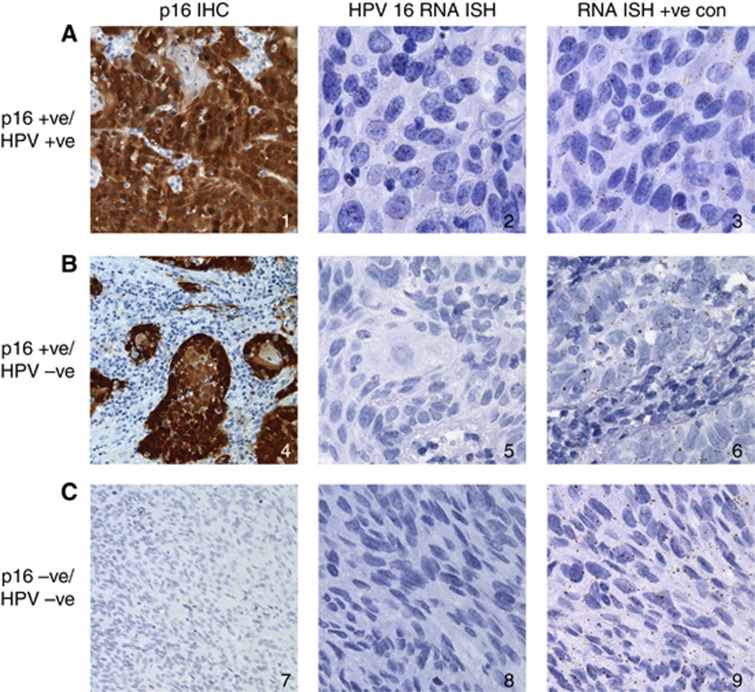
Methods: We evaluated a cohort of 324 laryngeal squamous cell carcinoma (LSCC) patients for the expression of p16(INK4A) (p16) protein by immunohistochemistry (IHC) and for high-risk HPV E6 and E7 mRNA transcripts by RNA in situ hybridisation (ISH). p16 expression and HPV status were correlated with clinicopathological features and outcomes.
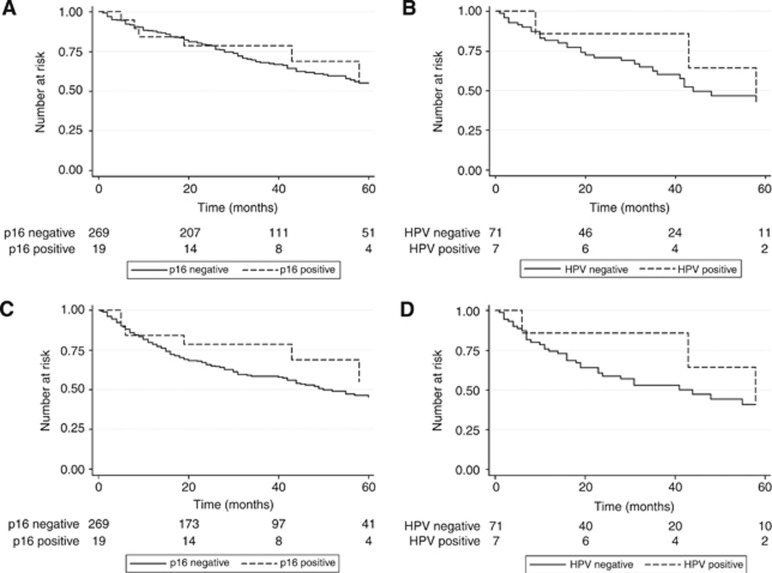
Results: Of 307 patients assessable for p16 IHC, 20 (6.5%) were p16 positive. Females and node-positive patients were more likely to be p16 positive (P<0.05). There were no other significant clinical or demographic differences between p16-positive and -negative cases. There was no difference in overall survival (OS) between p16-positive and -negative patients with 2-year survival of 79% in each group (HR=0.83, 95% CI 0.36-1.89, P=0.65). There was no statistically significant difference in failure-free survival (FFS) with 2-year FFS of 79% and 66% for p16-positive and -negative patients, respectively (HR=0.60, 95% CI 0.26-1.36, P=0.22). Only seven cases were found to be HPV RNA ISH positive, all of which were p16 IHC positive. There was no statistically significant difference in OS between patients with HPV RNA ISH-positive tumours compared with -negative tumours with 2-year survival of 86% and 71%, respectively (HR=0.76, 95% CI 0.23-2.5, P=0.65). The 2-year FFS was 86% and 59%, respectively (HR=0.62, 95% CI 0.19-2.03, P=0.43).
Conclusions: p16 overexpression is infrequent in LSCC and the proportion of cases with high-risk HPV transcripts is even lower. There are no statistically significant correlations between p16 IHC or HPV RNA ISH status and OS or disease outcomes.
Figures
Similar articles
-
Detection of transcriptionally active high-risk HPV in patients with head and neck squamous cell carcinoma as visualized by a novel E6/E7 mRNA in situ hybridization method.Am J Surg Pathol. 2012 Dec;36(12):1874-82. doi: 10.1097/PAS.0b013e318265fb2b. Am J Surg Pathol. 2012. PMID: 23060353 Free PMC article.
-
Verrucous carcinomas of the head and neck, including those with associated squamous cell carcinoma, lack transcriptionally active high-risk human papillomavirus.Hum Pathol. 2013 Nov;44(11):2385-92. doi: 10.1016/j.humpath.2013.07.011. Epub 2013 Sep 24. Hum Pathol. 2013. PMID: 24071016
-
Prostate tumor overexpressed-1, in conjunction with human papillomavirus status, predicts outcome in early-stage human laryngeal squamous cell carcinoma.Oncotarget. 2016 May 31;7(22):31878-91. doi: 10.18632/oncotarget.8103. Oncotarget. 2016. PMID: 26992242 Free PMC article.
-
Diagnostic accuracy of p16INK4a immunohistochemistry in oropharyngeal squamous cell carcinomas: A systematic review and meta-analysis.Int J Cancer. 2017 Mar 1;140(5):1186-1198. doi: 10.1002/ijc.30516. Epub 2016 Dec 2. Int J Cancer. 2017. PMID: 27859245
-
Correlation between human papillomavirus and p16 overexpression in oropharyngeal tumours: a systematic review.Br J Cancer. 2014 Mar 18;110(6):1587-94. doi: 10.1038/bjc.2014.42. Epub 2014 Feb 11. Br J Cancer. 2014. PMID: 24518594 Free PMC article.
Cited by
-
HPV Positive Status Is a Favorable Prognostic Factor in Non-Nasopharyngeal Head and Neck Squamous Cell Carcinoma Patients: A Retrospective Study From the Surveillance, Epidemiology, and End Results Database.Front Oncol. 2021 Sep 24;11:688615. doi: 10.3389/fonc.2021.688615. eCollection 2021. Front Oncol. 2021. PMID: 34631523 Free PMC article.
-
The prognostic role of sex, race, and human papillomavirus in oropharyngeal and nonoropharyngeal head and neck squamous cell cancer.Cancer. 2017 May 1;123(9):1566-1575. doi: 10.1002/cncr.30353. Epub 2017 Feb 27. Cancer. 2017. PMID: 28241096 Free PMC article.
-
HPV Meets APOBEC: New Players in Head and Neck Cancer.Int J Mol Sci. 2021 Jan 30;22(3):1402. doi: 10.3390/ijms22031402. Int J Mol Sci. 2021. PMID: 33573337 Free PMC article. Review.
-
Human papillomavirus and head and neck carcinomas: focus on evidence in the babel of published data.Acta Otorhinolaryngol Ital. 2016 Aug;36(4):249-258. doi: 10.14639/0392-100X-853. Acta Otorhinolaryngol Ital. 2016. PMID: 27734976 Free PMC article. Review.
-
Survival Outcomes in Human Papillomavirus-Associated Nonoropharyngeal Squamous Cell Carcinomas: A Systematic Review and Meta-analysis.JAMA Otolaryngol Head Neck Surg. 2020 Dec 1;146(12):1158-1166. doi: 10.1001/jamaoto.2020.3382. JAMA Otolaryngol Head Neck Surg. 2020. PMID: 33057610 Free PMC article.
References
-
- Baumann JL, Cohen S, Evjen AN, Law JH, Vadivelu S, Attia A, Schindler JS, Chung CH, Wirth PS, Meijer CJ, Snijders PJ, Yarbrough WG, Slebos RJ. Human papillomavirus in early laryngeal carcinoma. Laryngoscope. 2009;119 (8:1531–1537. - PubMed
-
- Bishop JA, Ma XJ, Wang H, Luo Y, Illei PB, Begum S, Taube JM, Koch WM, Westra WH. Detection of transcriptionally active high-risk HPV in patients with head and neck squamous cell carcinoma as visualized by a novel E6/E7 mRNA in situ hybridization method. Am J Surg Pathol. 2012;36 (12:1874–1882. - PMC - PubMed
-
- Bussu F, Sali M, Gallus R, Vellone VG, Zannoni GF, Autorino R, Dinapoli N, Santangelo R, Martucci R, Graziani C, Micciche F, Almadori G, Galli J, Delogu G, Sanguinetti M, Rindi G, Valentini V, Paludetti G. HPV infection in squamous cell carcinomas arising from different mucosal sites of the head and neck region. Is p16 immunohistochemistry a reliable surrogate marker. Br J Cancer. 2013;108 (5:1157–1162. - PMC - PubMed
-
- Chaturvedi AK, Engels EA, Pfeiffer RM, Hernandez BY, Xiao W, Kim E, Jiang B, Goodman MT, Sibug-Saber M, Cozen W, Liu L, Lynch CF, Wentzensen N, Jordan RC, Altekruse S, Anderson WF, Rosenberg PS, Gillison ML. Human papillomavirus and rising oropharyngeal cancer incidence in the United States. J Clin Oncol. 2011;29 (32:4294–4301. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
