

Twenty Percent of Patients May Remain Colonized With Methicillin-resistant Staphylococcus aureus Despite a Decolonization Protocol in Patients Undergoing Elective Total Joint Arthroplasty
- PMID: 25690169
- PMCID: PMC4457751
- DOI: 10.1007/s11999-015-4191-3
Twenty Percent of Patients May Remain Colonized With Methicillin-resistant Staphylococcus aureus Despite a Decolonization Protocol in Patients Undergoing Elective Total Joint Arthroplasty
Abstract
Background: Staphylococcus aureus is the most commonly isolated organism in periprosthetic joint infection (PJI). Resistant strains such as methicillin-resistant S aureus (MRSA) are on the rise, and many programs have instituted decolonization protocols. There are limited data on the success of S aureus nasal decolonization programs and their impact on PJI.
Questions/purposes: The purposes of this study were to (1) determine the proportion of patients successfully decolonized using a 2-week protocol; (2) compare infection risks between our surveillance and decolonization protocol group against a historical control cohort to evaluate changes in proportions of S aureus infections; and (3) assess infection risk based on carrier type, comparing S aureus carriers with noncarrier controls.
Methods: We retrospectively evaluated a group of 3434 patients who underwent elective primary and revision hip and knee arthroplasty over a 2-year period; each patient in the treatment group underwent a surveillance protocol, and a therapeutic regimen of mupurocin and chlorhexidine was instituted when colonization criteria were met. A 2009 to 2010 comparative historical cohort was chosen as the control group. We compared risks of infection between our treatment group and the historical control cohort. Furthermore, in patients who developed surgical site infections (SSIs), we compared the proportions of each S aureus type between the two cohorts. Finally, we compared infection rates based on carrier status. Surveillance for infection was carried out by the hospital infection control coordinator using the Centers for Disease Control and Prevention (CDC) criteria. During the time period of this study, the CDC defined hospital-acquired infection related to a surgical procedure as any infection diagnosed within 1 year of the procedure. With the numbers available, we had 41% power to detect a difference of 0.3% in infection rate between the treatment and control groups. To achieve 80% power, a total of 72,033 patients would be needed.
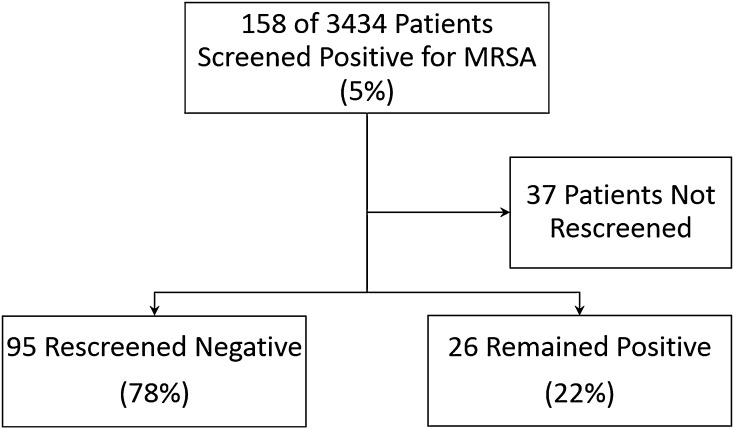
Results: Despite the protocol, 22% (26 of 121) of patients remained colonized with MRSA. With the numbers available, there were no differences in infection risk between the protocoled group (27 of 3434 [0.8%]) and the historical control group (33 of 3080 [1.1%]; relative risk [RR], 0.74; 95% confidence interval [CI], 0.44-1.22; p = 0.28). In terms of infecting organism in those who developed SSI, S aureus risk decreased slightly (treatment: 13 of 3434 patients [0.38%]; control: 21 of 3080 patients [0.68%]; RR, 0.56; CI, 0.28-1.11; p = 0.11). Within the protocoled group, carriers had a slightly higher risk of developing SSI (carrier: seven of 644 [1.1%]; noncarrier: 18 of 2763 [0.65%]; RR, 1.77; CI, 0.74-4.24; p = 0.20).
Conclusions: The screening and decolonization protocol enabled a substantial reduction in nasal carriage of MRSA, but some patients remained colonized. However, our nasal decolonization protocol before elective total joint arthroplasty did not demonstrate a decrease in the proportion of patients developing SSI. Future meta-analyses and systematic reviews will be needed to pool the results of studies like these to ascertain whether small improvements in infection risk are achieved by protocols like ours and to determine whether any such improvements warrant the costs and potential risks of surveillance and intervention.
Level of evidence: Level III, therapeutic study.
Figures
References
-
- Bode LG, Wertheim HF, Kluytmans JA, Bogaers-Hofman D, Vandenbroucke-Grauls CM, Roosendaal R, Toelstra A, Box AT, Voss A, van Belkum A, Verbrugh HA, Vos MC. Preventing surgical-site infections in nasal carriers of Staphylococcus aureus. N Engl J Med. 2010;362:9–17. doi: 10.1056/NEJMoa0808939. - DOI - PubMed
-
- Bradbury T, Fehring TK, Taunton M, Hanssen A, Azzam K, Parvizi J, Odum SM. The Fate of acute methicillin-resistant Staphylococcus aureus periprosthetic knee infections treated by open débridement and retention of components. J Arthroplasty. 2009;24:101–104. doi: 10.1016/j.arth.2009.04.028. - DOI - PubMed
-
- Climo MW, Sepkowitz KA, Zuccotti G, Fraser VJ, Warren DK, Perl TM, Speck K, Jernigan JA, Robles JR, Wong ES. The effect of daily bathing with chlorhexidine on the acquisition of methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococcus, and healthcare-associated bloodstream infections: results of a quasi-experimental multicenter trial. Crit Care Med. 2009;37:1858–1865. doi: 10.1097/CCM.0b013e31819ffe6d. - DOI - PubMed
-
- Deshpande LM, Fix AM, Pfaller MA, Jones RN, SENTRY Antimicrobial Surveillance Program Participants Group Emerging elevated mupirocin resistance rates among staphylococcal isolates in the SENTRY Antimicrobial Surveillance Program (2000): correlations of results from disk diffusion, Etest and reference dilution methods. Diagn Microbiol Infect Dis. 2000;2002(42):283–290. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
