

Development and validation of a risk stratification score for ventral incisional hernia after abdominal surgery: hernia expectation rates in intra-abdominal surgery (the HERNIA Project)
- PMID: 25690673
- PMCID: PMC4372474
- DOI: 10.1016/j.jamcollsurg.2014.12.027
Development and validation of a risk stratification score for ventral incisional hernia after abdominal surgery: hernia expectation rates in intra-abdominal surgery (the HERNIA Project)
Abstract
Background: Ventral incisional hernias (VIH) develop in up to 20% of patients after abdominal surgery. No widely applicable preoperative risk-assessment tool exists. We aimed to develop and validate a risk-assessment tool to predict VIH after abdominal surgery.
Study design: A prospective study of all patients undergoing abdominal surgery was conducted at a single institution from 2008 to 2010. Variables were defined in accordance with the National Surgical Quality Improvement Project, and VIH was determined through clinical and radiographic evaluation. A multivariate Cox proportional hazard model was built from a development cohort (2008 to 2009) to identify predictors of VIH. The HERNIAscore was created by converting the hazards ratios (HR) to points. The predictive accuracy was assessed on the validation cohort (2010) using a receiver operator characteristic curve and calculating the area under the curve (AUC).
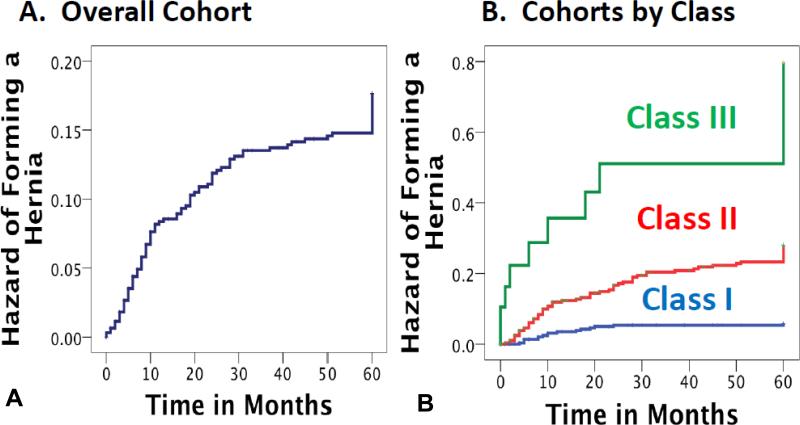
Results: Of 625 patients followed for a median of 41 months (range 0.3 to 64 months), 93 (13.9%) developed a VIH. The training cohort (n = 428, VIH = 70, 16.4%) identified 4 independent predictors: laparotomy (HR 4.77, 95% CI 2.61 to 8.70) or hand-assisted laparoscopy (HAL, HR 4.00, 95% CI 2.08 to 7.70), COPD (HR 2.35; 95% CI 1.44 to 3.83), and BMI ≥ 25 kg/m(2) (HR1.74; 95% CI 1.04 to 2.91). Factors that were not predictive included age, sex, American Society of Anesthesiologists (ASA) score, albumin, immunosuppression, previous surgery, and suture material or technique. The predictive score had an AUC = 0.77 (95% CI 0.68 to 0.86) using the validation cohort (n = 197, VIH = 23, 11.6%). Using the HERNIAscore: HERNIAscore = 4(∗)Laparotomy+3(∗)HAL+1(∗)COPD+1(∗) BMI ≥ 25, 3 classes stratified the risk of VIH: class I (0 to 3 points),5.2%; class II (4 to 5 points),19.6%; and class III (6 points), 55.0%.
Conclusions: The HERNIAscore accurately identifies patients at increased risk for VIH. Although external validation is needed, this provides a starting point to counsel patients and guide clinical decisions. Increasing the use of laparoscopy, weight-loss programs, community smoking prevention programs, and incisional reinforcement may help reduce rates of VIH.
Copyright © 2015 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Discussion.J Am Coll Surg. 2015 Apr;220(4):413-5. doi: 10.1016/j.jamcollsurg.2015.01.008. J Am Coll Surg. 2015. PMID: 25797723 No abstract available.
References
-
- Nunoo-Mensah JW, Rosen M, Chan LS, et al. Prevalence of intra-abdominal surgery: what is an individual's lifetime risk? South Med J. 2009;102:25–29. - PubMed
-
- van Ramshorst GH, Eker HH, Hop WC, et al. Impact of incisional hernia on health-related quality of life and body image: a prospective cohort study. Am J Surg. 2012;204(2):144–50. - PubMed
-
- Li LT, Jafrani RJ, Becker NS, et al. Outcomes of acute versus elective primary ventral hernia repair. J Trauma Acute Care Surg. 2014;76(2):523–8. - PubMed
-
- Berger RL, Li LT, Hicks SC, et al. Development and validation of a risk-stratification score for surgical site occurrence and surgical site infection after open ventral hernia repair. J Am Coll Surg. 2013;217(6):974–82. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
