

Outdoor temperature, blood pressure, and cardiovascular disease mortality among 23 000 individuals with diagnosed cardiovascular diseases from China
- PMID: 25690792
- PMCID: PMC4430682
- DOI: 10.1093/eurheartj/ehv023
Outdoor temperature, blood pressure, and cardiovascular disease mortality among 23 000 individuals with diagnosed cardiovascular diseases from China
Abstract
Introduction: Blood pressure is a major cause of cardiovascular disease (CVD) and both may increase as outdoor temperatures fall. However, there are still limited data about seasonal variation in blood pressure and CVD mortality among patients with prior-CVD.
Methods: We analysed data on 23 000 individuals with prior-CVD who were recruited from 10 diverse regions into the China Kadoorie Biobank during 2004-8. After 7 years of follow-up, 1484 CVD deaths were recorded. Baseline survey data were used to assess seasonal variation in systolic blood pressure (SBP) and its association with outdoor temperature. Cox regression was used to examine the association of usual SBP with subsequent CVD mortality, and seasonal variation in CVD mortality was assessed by Poisson regression. All analyses were adjusted for age, sex, and region.
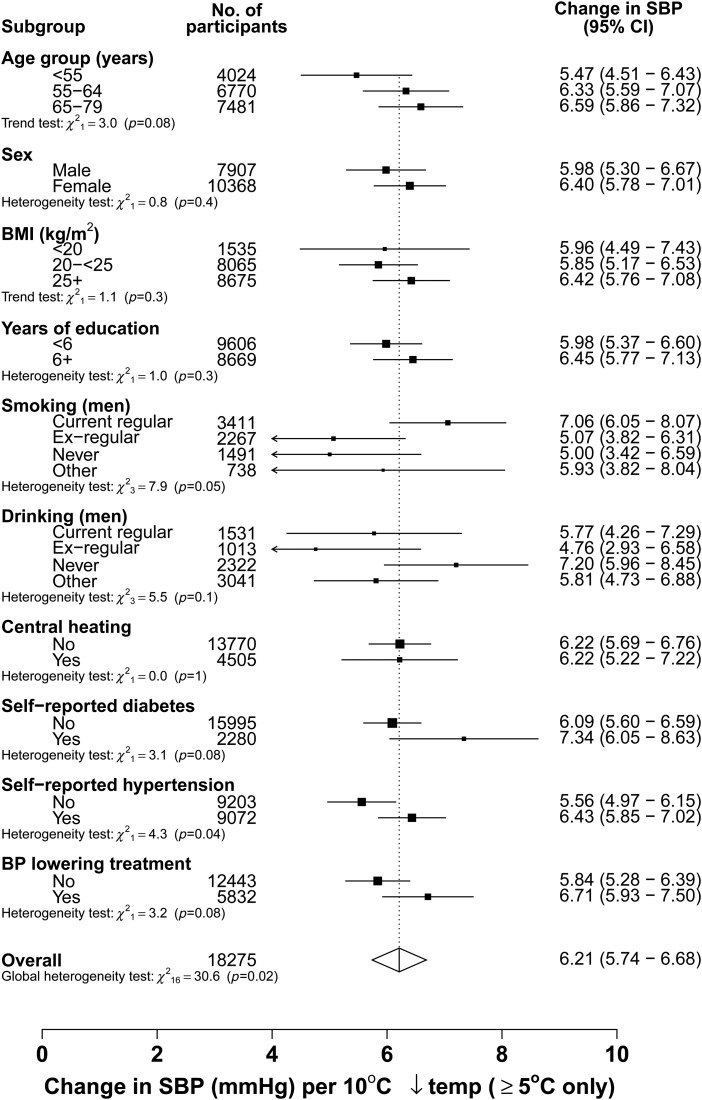
Results: Mean SBP was significantly higher in winter than in summer (145 vs. 136 mmHg, P < 0.001), especially among those without central heating. Above 5°C, each 10°C lower outdoor temperature was associated with 6.2 mmHg higher SBP. Systolic blood pressure predicted subsequent CVD mortality, with each 10 mmHg higher usual SBP associated with 21% (95% confidence interval: 16-27%) increased risk. Cardiovascular disease mortality varied by season, with 41% (21-63%) higher risk in winter compared with summer.
Conclusion: Among adult Chinese with prior-CVD, there is both increased blood pressure and CVD mortality in winter. Careful monitoring and more aggressive blood pressure lowering treatment in the cold months are needed to help reduce the winter excess CVD mortality in high-risk individuals.
Keywords: Blood pressure; Cardiovascular disease; China; Cohort study; Hypertension; Seasonal variation.
© The Author 2015. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures





Comment in
-
' 'tis bitter cold and I am sick at heart': establishing the relationship between outdoor temperature, blood pressure, and cardiovascular mortality.Eur Heart J. 2015 May 14;36(19):1152-4. doi: 10.1093/eurheartj/ehv024. Epub 2015 Mar 8. Eur Heart J. 2015. PMID: 25755114 No abstract available.
References
-
- WHO. Cardiovascular diseases (CVDS) http://www.Who.Int/mediacentre/factsheets/fs317/en/ 2013.
-
- Chen Z. The third national retrospective sampling mortality survey report. Beijing: China Union Medical University Publishing House; 2008.
-
- Yang G, Kong L, Zhao W, Wan X, Zhai Y, Chen LC, Koplan JP. Emergence of chronic non-communicable diseases in China. Lancet 2008;372:1697–1705. - PubMed
-
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002;360:1903–1913. - PubMed
-
- He J, Gu D, Chen J, Wu X, Kelly TN, Huang JF, Chen JC, Chen CS, Bazzano LA, Reynolds K, Whelton PK, Klag MJ. Premature deaths attributable to blood pressure in China: a prospective cohort study. Lancet 2009;374:1765–1772. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
