

Case characteristics, hyperacute treatment, and outcome information from the clinical research center for stroke-fifth division registry in South Korea
- PMID: 25692106
- PMCID: PMC4325643
- DOI: 10.5853/jos.2015.17.1.38
Case characteristics, hyperacute treatment, and outcome information from the clinical research center for stroke-fifth division registry in South Korea
Erratum in
-
ERRATUM: Table Correction: Case Characteristics, Hyperacute Treatment, and Outcome Information from the Clinical Research Center for Stroke-Fifth Division Registry in South Korea.J Stroke. 2015 Sep;17(3):377-8. doi: 10.5853/jos.2015.17.3.377. J Stroke. 2015. PMID: 26438006 Free PMC article. No abstract available.
Abstract
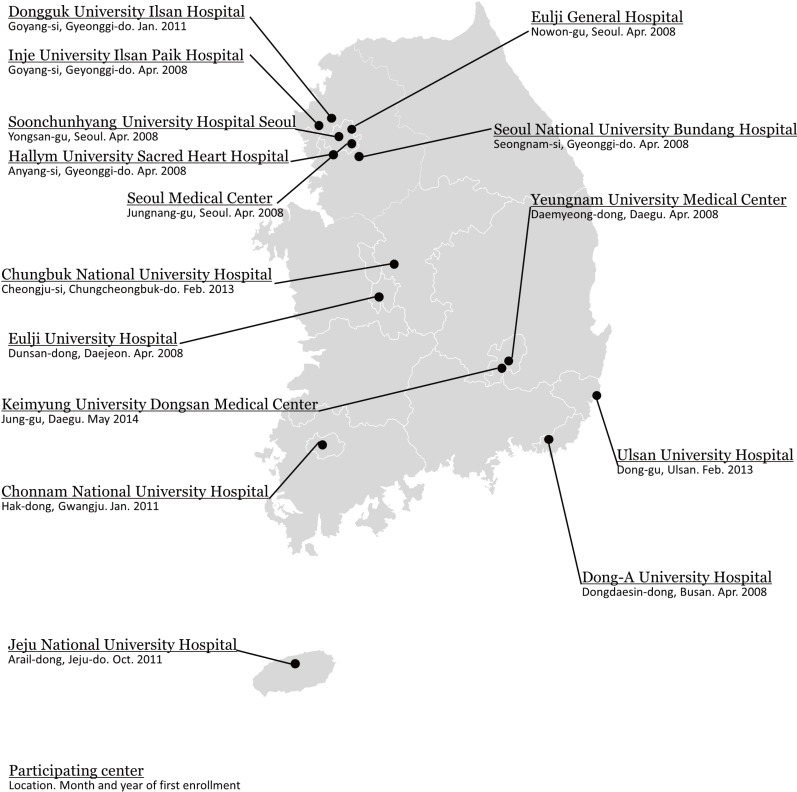
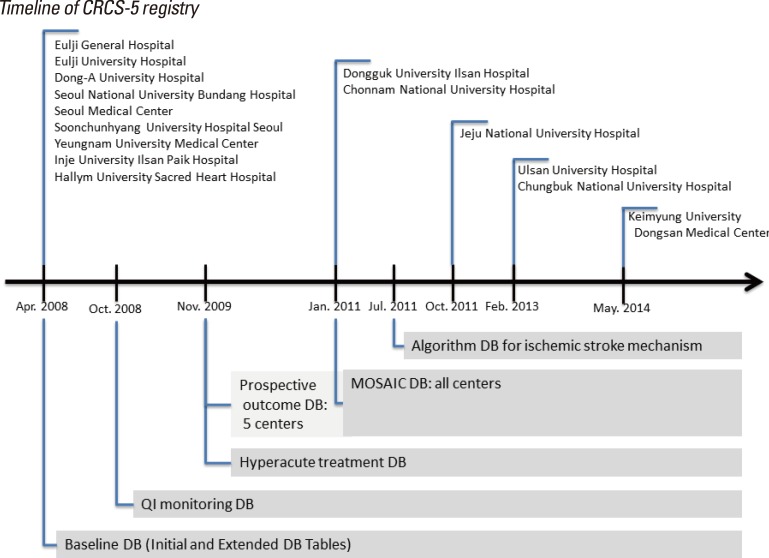
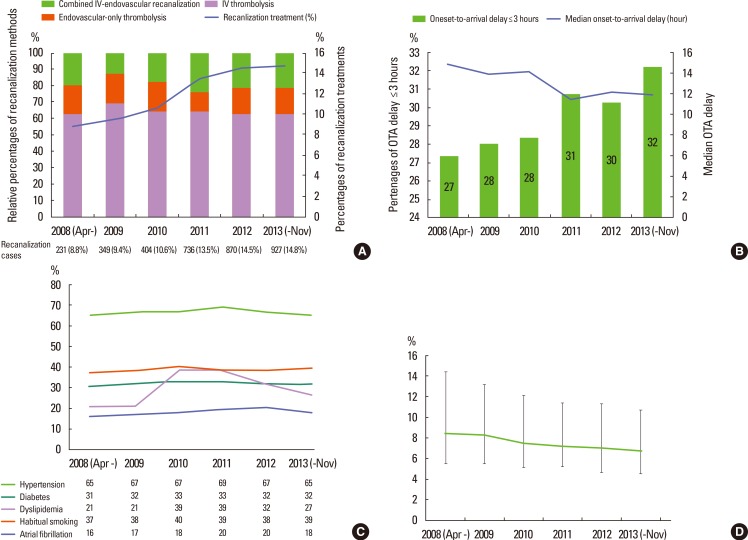
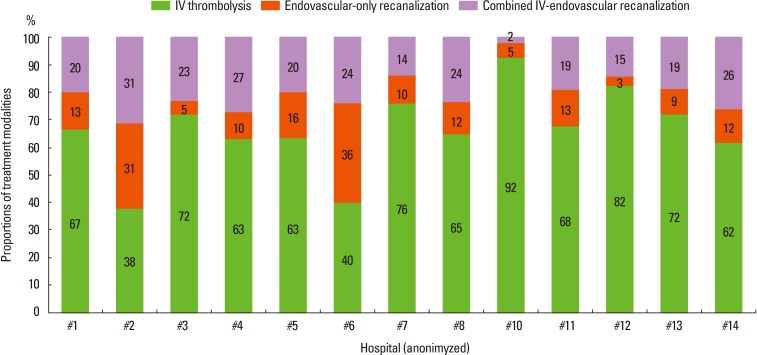
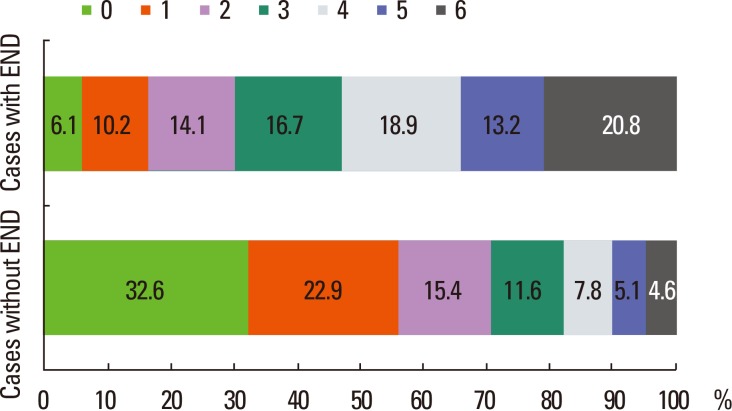
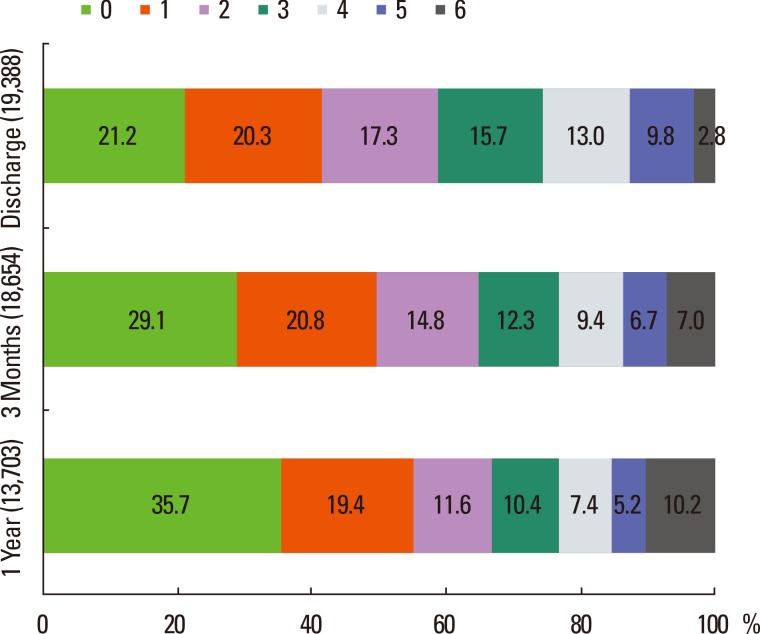
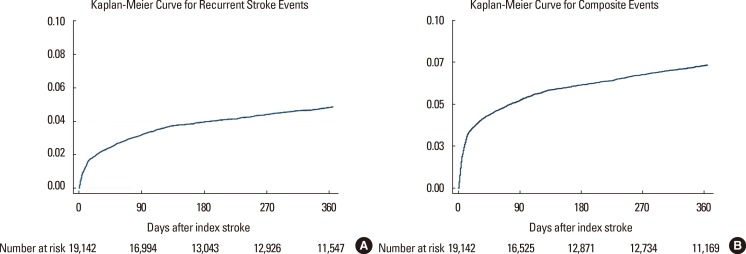
Characteristics of stroke cases, acute stroke care, and outcomes after stroke differ according to geographical and cultural background. To provide epidemiological and clinical data on stroke care in South Korea, we analyzed a prospective multicenter clinical stroke registry, the Clinical Research Center for Stroke-Fifth Division (CRCS-5). Patients were 58% male with a mean age of 67.2±12.9 years and median National Institutes of Health Stroke Scale score of 3 [1-8] points. Over the 6 years of operation, temporal trends were documented including increasing utilization of recanalization treatment with shorter onset-to-arrival delay and decremental length of stay. Acute recanalization treatment was performed in 12.7% of cases with endovascular treatment utilized in 36%, but the proportion of endovascular recanalization varied across centers. Door-to-IV alteplase delay had a median of 45 [33-68] min. The rate of symptomatic hemorrhagic transformation (HT) was 7%, and that of any HT was 27% among recanalization-treated cases. Early neurological deterioration occurred in 15% of cases and were associated with longer length of stay and poorer 3-month outcomes. The proportion of mRS scores of 0-1 was 42% on discharge, 50% at 3 months, and 55% at 1 year after the index stroke. Recurrent stroke up to 1 year occurred in 4.5% of patients; the rate was higher among older individuals and those with neurologically severe deficits. The above findings will be compared with other Asian and US registry data in this article.
Keywords: Case profile; Hyperacute treatment; Outcome; Recurrent event; South Korea; Stroke registry; Thrombolysis.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Bufalino VJ, Masoudi FA, Stranne SK, Horton K, Albert NM, Beam C, et al. The American Heart Association's recommendations for expanding the applications of existing and future clinical registries: a policy statement from the American Heart Association. Circulation. 2011;123:2167–2179. - PubMed
-
- Gliklich RE, Dreyer NA. Registries for Evaluating Patient Outcomes: A User's Guide. 2nd ed. Rockville (MD): Agency for Healthcare Research and Quality (US); 2010. - PubMed
-
- Maasland L, van Oostenbrugge RJ, Franke CF, Scholte Op Reimer WJM, Koudstaal PJ, et al. Patients enrolled in large randomized clinical trials of antiplatelet treatment for prevention after transient ischemic attack or ischemic stroke are not representative of patients in clinical practice: the Netherlands Stroke Survey. Stroke. 2009;40:2662–2668. - PubMed
-
- Lee BC, Roh JK. International Experience in Stroke Registries. Am J Prev Med. 2006;31:S243–S245. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
