

Sociodemographic and geographic predictors of quality of care in United States patients with end-stage renal disease due to lupus nephritis
- PMID: 25692867
- PMCID: PMC5340148
- DOI: 10.1002/art.38983
Sociodemographic and geographic predictors of quality of care in United States patients with end-stage renal disease due to lupus nephritis
Abstract
Objective: To describe end-stage renal disease (ESRD) quality of care (receipt of pre-ESRD nephrology care, access to kidney transplantation, and placement of permanent vascular access for dialysis) in US patients with ESRD due to lupus nephritis (LN-ESRD) and to examine whether quality measures differ by patient sociodemographic characteristics or US region.
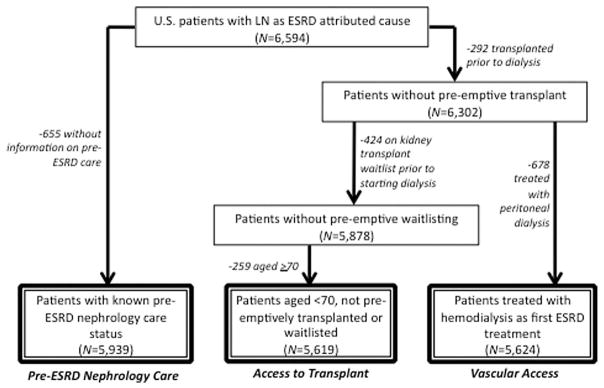
Methods: National surveillance data on patients in the US in whom treatment for LN-ESRD was initiated between July 2005 and September 2011 (n = 6,594) were analyzed. Odds ratios (ORs) and hazard ratios (HRs) with 95% confidence intervals (95% CIs) were determined for each quality measure, according to sociodemographic factors and US region.
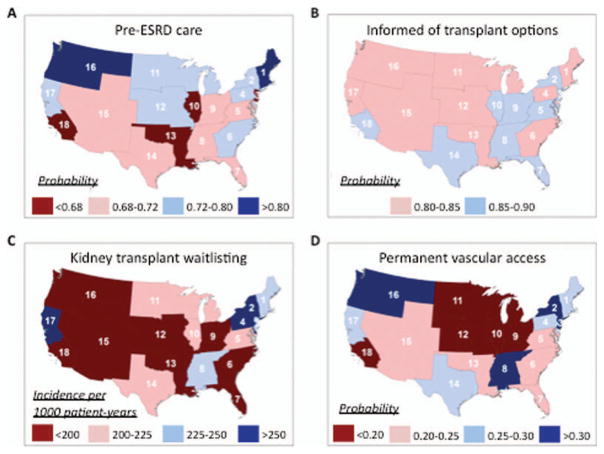
Results: Overall, 71% of the patients received nephrology care prior to ESRD. Black and Hispanic patients were less likely than white patients to receive pre-ESRD care (OR 0.73 [95% CI 0.63-0.85] and OR 0.73 [95% CI 0.60-0.88], respectively) and to be placed on the kidney transplant waitlist within the first year after the start of ESRD (HR 0.78 [95% CI 0.68-0.91] and HR 0.82 [95% CI 0.68-0.98], respectively). Those with Medicaid (HR 0.51 [95% CI 0.44-0.58]) or no insurance (HR 0.36 [95% CI 0.29-0.44]) were less likely than those with private insurance to be placed on the waitlist. Only 24% had a permanent vascular access, and placement was even less likely among the uninsured (OR 0.62 [95% CI 0.49-0.79]). ESRD quality-of-care measures varied 2-3-fold across regions of the US, with patients in the Northeast and Northwest generally having higher probabilities of adequate care.
Conclusion: LN-ESRD patients have suboptimal ESRD care, particularly with regard to placement of dialysis vascular access. Minority race/ethnicity and lack of private insurance are associated with inadequate ESRD care. Further studies are warranted to examine multilevel barriers to, and develop targeted interventions to improve delivery of, care among patients with LN-ESRD.
Copyright © 2015 by the American College of Rheumatology.
Figures
References
-
- Centers for Medicare & Medicaid Services, US Department of Health and Human Services. Medicare program: end-stage renal disease prospective payment system for calendar year 2014. Federal Register. 2013 Dec 2;38(231) CMS-1526-F http://www.gpo.gov/fdsys/pkg/FR-2013-12-02/pdf/2013-28451.pdf.
-
- Office of Disease Prevention and Health Promotion, US Department of Health and Human Services. Healthy people 2020. www.healthypeople.gov.
-
- Astor BC, Eustace JA, Powe NR, Klag MJ, Sadler JH, Fink NE, et al. Timing of nephrologist referral and arteriovenous access use: the CHOICE Study. Am J Kidney Dis. 2001;38:494–501. - PubMed
-
- Avorn J, Winkelmayer WC, Bohn RL, Levin R, Glynn RJ, Levy E, et al. Delayed nephrologist referral and inadequate vascular access in patients with advanced chronic kidney failure. J Clin Epidemiol. 2002;55:711–6. - PubMed
-
- Winkelmayer WC, Glynn RJ, Levin R, Owen W, Jr, Avorn J. Late referral and modality choice in end-stage renal disease. Kidney Int. 2001;60:1547–54. - PubMed
Publication types
MeSH terms
Grants and funding
- KL2-TR-000455/TR/NCATS NIH HHS/United States
- R01 AR065493/AR/NIAMS NIH HHS/United States
- KL2 TR000455/TR/NCATS NIH HHS/United States
- K01 HD074726/HD/NICHD NIH HHS/United States
- R01-AR-065493/AR/NIAMS NIH HHS/United States
- K01-HD-074726/HD/NICHD NIH HHS/United States
- U01-DP-005119/DP/NCCDPHP CDC HHS/United States
- ULL-TR-000454/TR/NCATS NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- U01 DP006488/DP/NCCDPHP CDC HHS/United States
- R24 MD008077/MD/NIMHD NIH HHS/United States
- U01DP005119/ACL/ACL HHS/United States
- 1R24-MD-008077-01/MD/NIMHD NIH HHS/United States
- U01 DP005119/DP/NCCDPHP CDC HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
