

Early changes in liver distribution following implementation of Share 35
- PMID: 25693474
- PMCID: PMC6116537
- DOI: 10.1111/ajt.13099
Early changes in liver distribution following implementation of Share 35
Abstract
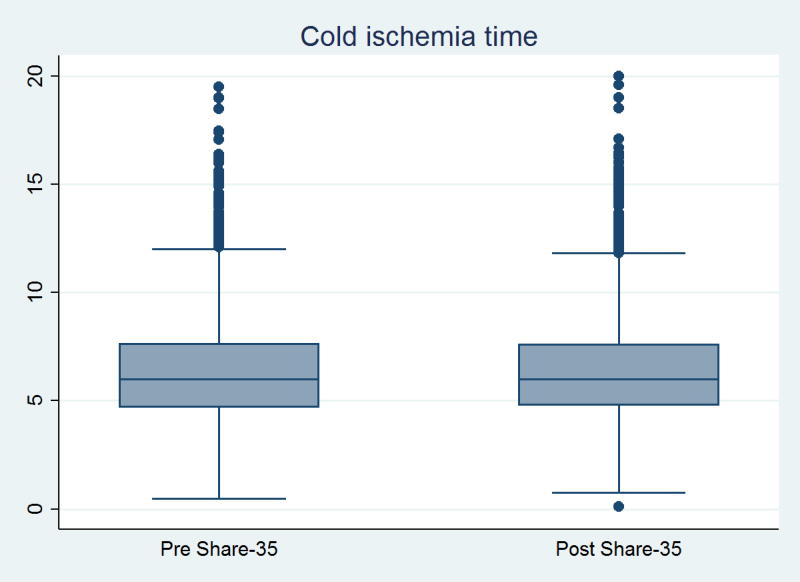
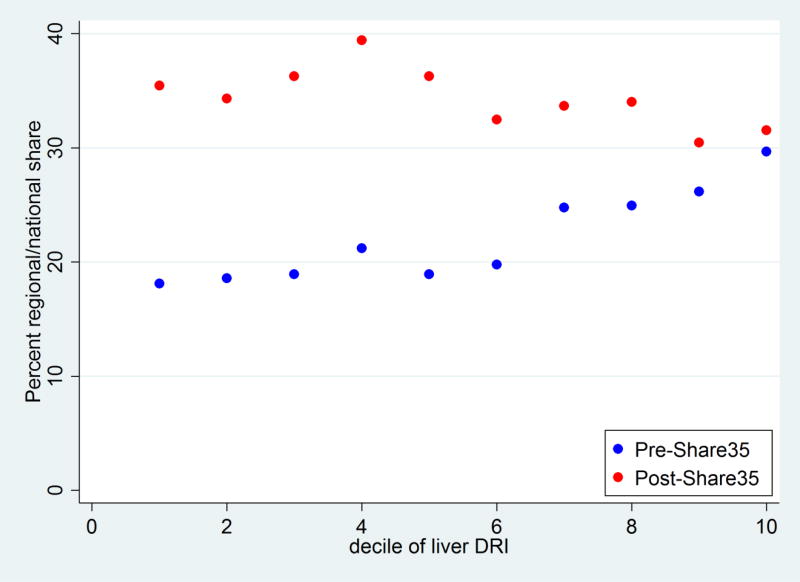
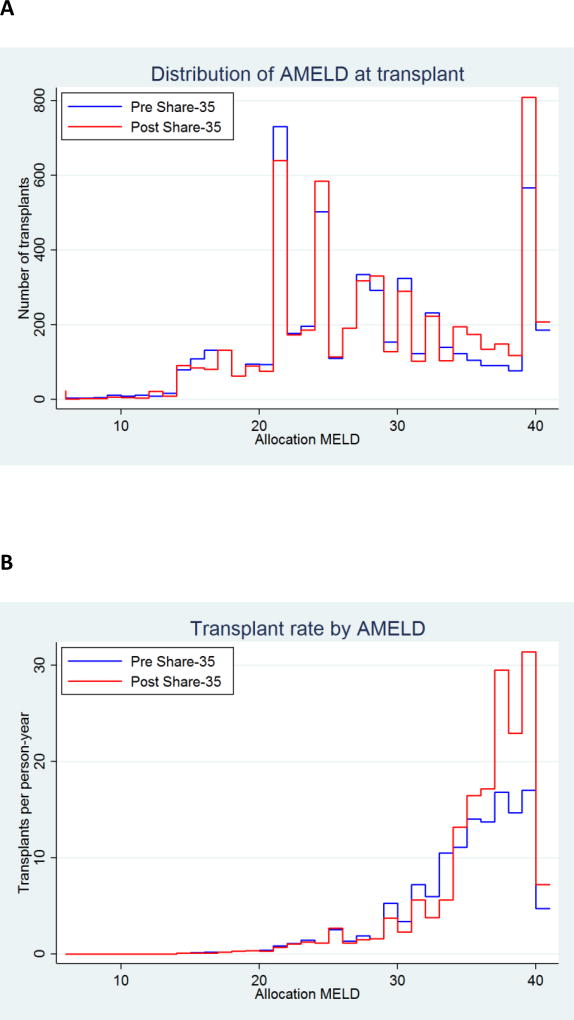
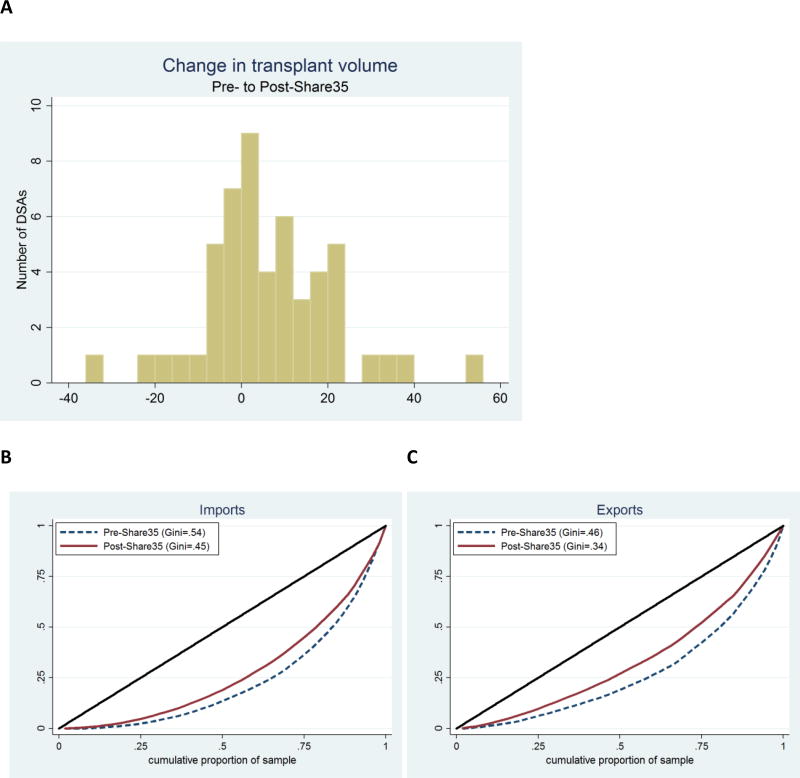
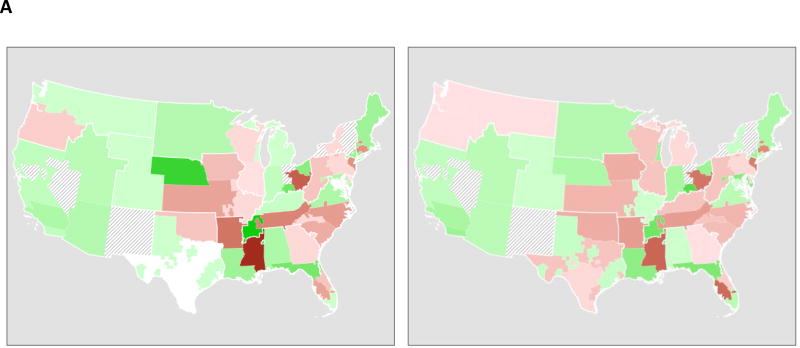
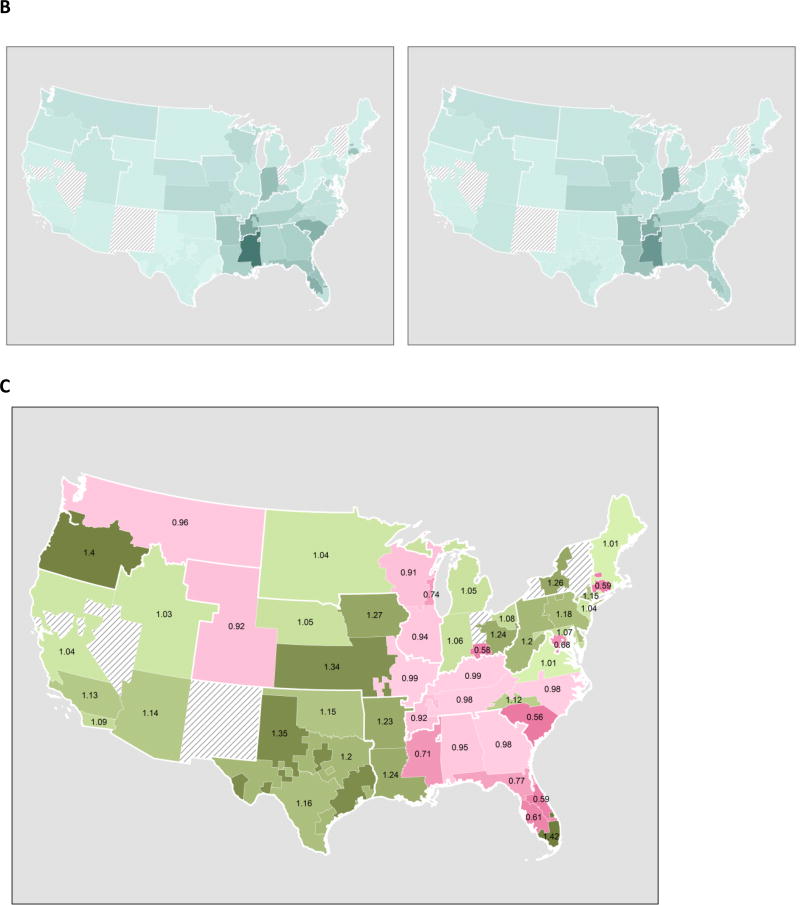
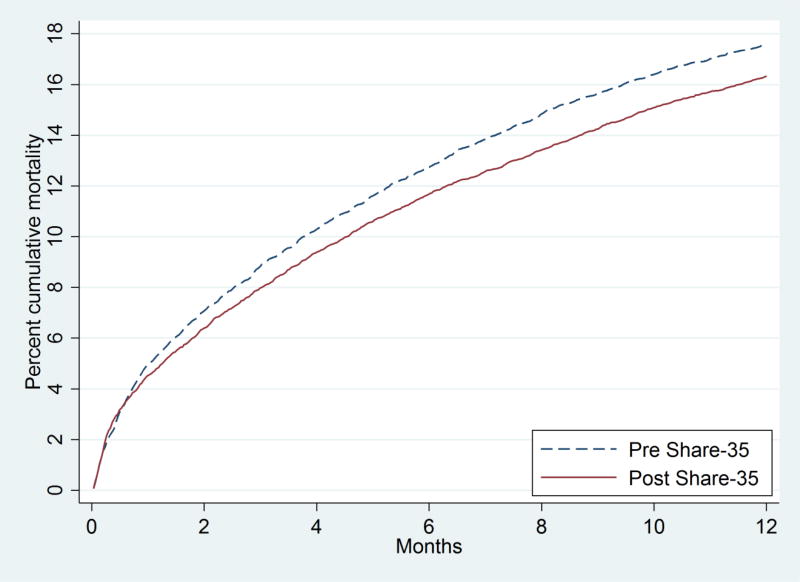
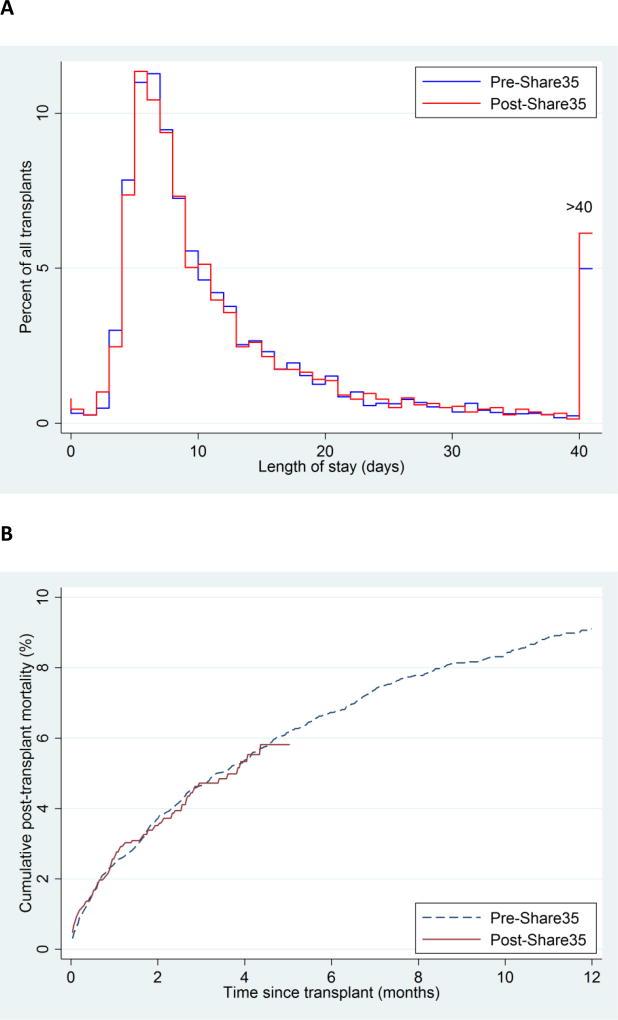
In June 2013, a change to the liver waitlist priority algorithm was implemented. Under Share 35, regional candidates with MELD ≥ 35 receive higher priority than local candidates with MELD < 35. We compared liver distribution and mortality in the first 12 months of Share 35 to an equivalent time period before. Under Share 35, new listings with MELD ≥ 35 increased slightly from 752 (9.2% of listings) to 820 (9.7%, p = 0.3), but the proportion of deceased-donor liver transplants (DDLTs) allocated to recipients with MELD ≥ 35 increased from 23.1% to 30.1% (p < 0.001). The proportion of regional shares increased from 18.9% to 30.4% (p < 0.001). Sharing of exports was less clustered among a handful of centers (Gini coefficient decreased from 0.49 to 0.34), but there was no evidence of change in CIT (p = 0.8). Total adult DDLT volume increased from 4133 to 4369, and adjusted odds of discard decreased by 14% (p = 0.03). Waitlist mortality decreased by 30% among patients with baseline MELD > 30 (SHR = 0.70, p < 0.001) with no change for patients with lower baseline MELD (p = 0.9). Posttransplant length-of-stay (p = 0.2) and posttransplant mortality (p = 0.9) remained unchanged. In the first 12 months, Share 35 was associated with more transplants, fewer discards, and lower waitlist mortality, but not at the expense of CIT or early posttransplant outcomes.
Keywords: United Network for Organ Sharing (UNOS); epidemiology; ethics and public policy; health services and outcomes research; liver transplantation/hepatology; organ allocation; organ procurement and allocation; social sciences.
© Copyright 2015 The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
The authors of this manuscript have no conflicts of interest to disclose as described by the American Journal of Transplantation.
Figures
References
-
- Washburn K, Pomfret E, Roberts J. Liver allocation and distribution: possible next steps. Liver transplantation : official publication of the American Association for the Study of Liver Diseases and the International Liver Transplantation Society. 2011;17(9):1005–1012. - PubMed
-
- Leppke S, Leighton T, Zaun D, Chen SC, Skeans M, Israni AK, et al. Scientific Registry of Transplant Recipients: collecting, analyzing, and reporting data on transplantation in the United States. Transplant Rev (Orlando) 2013;27(2):50–56. - PubMed
-
- Massie AB, Caffo B, Gentry SE, Hall EC, Axelrod DA, Lentine KL, et al. MELD Exceptions and Rates of Waiting List Outcomes. American journal of transplantation : official journal of the American Society of Transplantation and the American Society of Transplant Surgeons. 2011;11(11):2362–2371. - PMC - PubMed
-
- Feng S, Goodrich NP, Bragg-Gresham JL, Dykstra DM, Punch JD, DebRoy MA, et al. Characteristics associated with liver graft failure: the concept of a donor risk index. American journal of transplantation : official journal of the American Society of Transplantation and the American Society of Transplant Surgeons. 2006;6(4):783–790. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
