

Prevalence and prognosis of Alzheimer's disease at the mild cognitive impairment stage
- PMID: 25693589
- PMCID: PMC5013930
- DOI: 10.1093/brain/awv029
Prevalence and prognosis of Alzheimer's disease at the mild cognitive impairment stage
Abstract
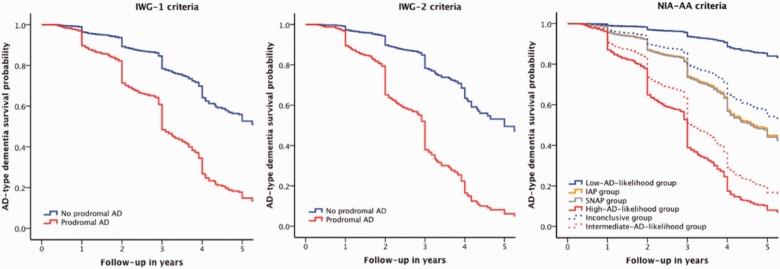
Three sets of research criteria are available for diagnosis of Alzheimer's disease in subjects with mild cognitive impairment: the International Working Group-1, International Working Group-2, and National Institute of Aging-Alzheimer Association criteria. We compared the prevalence and prognosis of Alzheimer's disease at the mild cognitive impairment stage according to these criteria. Subjects with mild cognitive impairment (n = 1607), 766 of whom had both amyloid and neuronal injury markers, were recruited from 13 cohorts. We used cognitive test performance and available biomarkers to classify subjects as prodromal Alzheimer's disease according to International Working Group-1 and International Working Group-2 criteria and in the high Alzheimer's disease likelihood group, conflicting biomarker groups (isolated amyloid pathology or suspected non-Alzheimer pathophysiology), and low Alzheimer's disease likelihood group according to the National Institute of Ageing-Alzheimer Association criteria. Outcome measures were the proportion of subjects with Alzheimer's disease at the mild cognitive impairment stage and progression to Alzheimer's disease-type dementia. We performed survival analyses using Cox proportional hazards models. According to the International Working Group-1 criteria, 850 (53%) subjects had prodromal Alzheimer's disease. Their 3-year progression rate to Alzheimer's disease-type dementia was 50% compared to 21% for subjects without prodromal Alzheimer's disease. According to the International Working Group-2 criteria, 308 (40%) subjects had prodromal Alzheimer's disease. Their 3-year progression rate to Alzheimer's disease-type dementia was 61% compared to 22% for subjects without prodromal Alzheimer's disease. According to the National Institute of Ageing-Alzheimer Association criteria, 353 (46%) subjects were in the high Alzheimer's disease likelihood group, 49 (6%) in the isolated amyloid pathology group, 220 (29%) in the suspected non-Alzheimer pathophysiology group, and 144 (19%) in the low Alzheimer's disease likelihood group. The 3-year progression rate to Alzheimer's disease-type dementia was 59% in the high Alzheimer's disease likelihood group, 22% in the isolated amyloid pathology group, 24% in the suspected non-Alzheimer pathophysiology group, and 5% in the low Alzheimer's disease likelihood group. Our findings support the use of the proposed research criteria to identify Alzheimer's disease at the mild cognitive impairment stage. In clinical settings, the use of both amyloid and neuronal injury markers as proposed by the National Institute of Ageing-Alzheimer Association criteria offers the most accurate prognosis. For clinical trials, selection of subjects in the National Institute of Ageing-Alzheimer Association high Alzheimer's disease likelihood group or the International Working Group-2 prodromal Alzheimer's disease group could be considered.
Keywords: Alzheimer’s disease; MCI; biomarkers; diagnostic criteria; prognosis.
© The Author (2015). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures

Comment in
-
New criteria for Alzheimer's disease: which, when and why?Brain. 2015 May;138(Pt 5):1134-7. doi: 10.1093/brain/awv055. Brain. 2015. PMID: 25907755 Free PMC article.
References
-
- American Psychiatric Association. Washington, DC: American Psychiatric Association; 1994. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV.
-
- Baldeiras I, Santana I, Proença MT, Garrucho MH, Pascoal R, Rodrigues A, et al. Peripheral oxidative damage in mild cognitive impairment and mild Alzheimer’s disease. J Alzheimers Dis. 2008;15:117–28. - PubMed
-
- Bastin C, Kerrouche N, Lekeu F, Adam S, Guillaume B, Lemaire C, et al. Controlled memory processes in questionable Alzheimer's disease: a view from neuroimaging research. J Alzheimers Dis. 2010;20:547–60. - PubMed
-
- Bouwman FH, Verwey NA, Klein M, Kok A, Blankenstein MA, Sluimer JD, et al. New research criteria for the diagnosis of Alzheimer’s disease applied in a memory clinic population. Dement Geriatr Cogn Disord. 2010;30:1–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
