

Antidepressant use and risk of suicide and attempted suicide or self harm in people aged 20 to 64: cohort study using a primary care database
- PMID: 25693810
- PMCID: PMC4353276
- DOI: 10.1136/bmj.h517
Antidepressant use and risk of suicide and attempted suicide or self harm in people aged 20 to 64: cohort study using a primary care database
Abstract
Objective: To assess the associations between different antidepressant treatments and the rates of suicide and attempted suicide or self harm in people with depression.
Design: Cohort study.
Setting: Patients registered with UK general practices contributing data to the QResearch database.
Participants: 238,963 patients aged 20 to 64 years with a first diagnosis of depression between 1 January 2000 and 31 July 2011, followed up until 1 August 2012.
Exposures: Antidepressant class (tricyclic and related antidepressants, selective serotonin reuptake inhibitors, other antidepressants), dose, and duration of use, and commonly prescribed individual antidepressant drugs. Cox proportional hazards models were used to calculate hazard ratios adjusting for potential confounding variables.
Main outcome measures: Suicide and attempted suicide or self harm during follow-up.
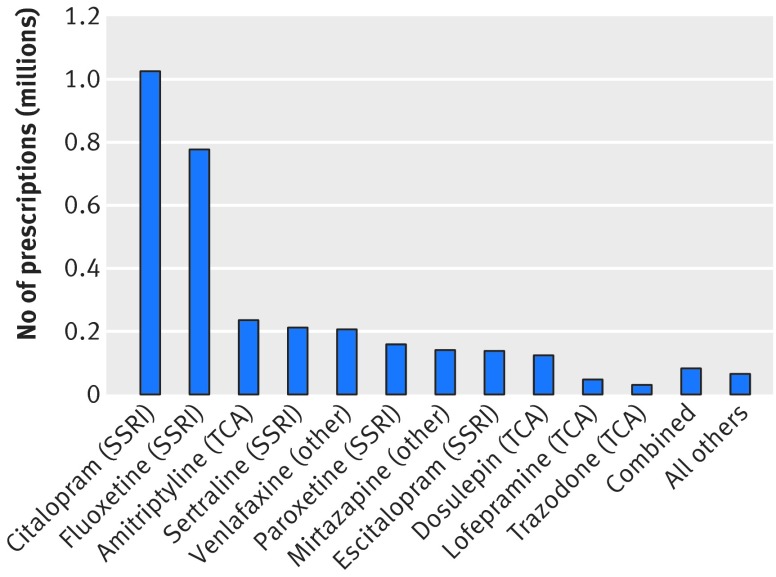
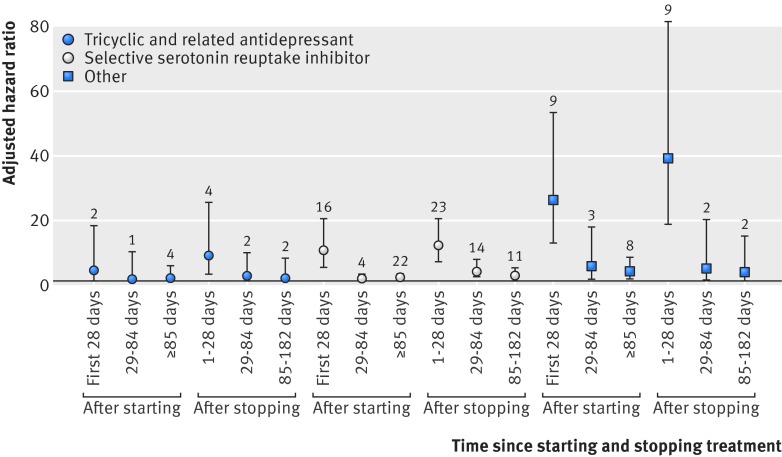
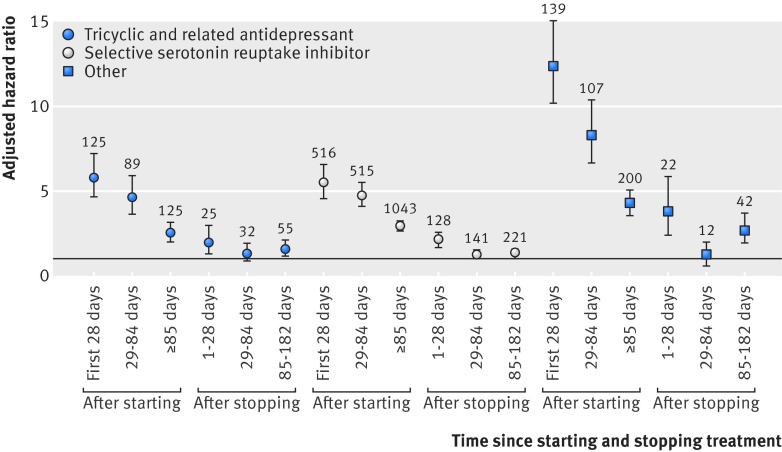
Results: During follow-up, 87.7% (n = 209,476) of the cohort received one or more prescriptions for antidepressants. The median duration of treatment was 221 days (interquartile range 79-590 days). During the first five years of follow-up 198 cases of suicide and 5243 cases of attempted suicide or self harm occurred. The difference in suicide rates during periods of treatment with tricyclic and related antidepressants compared with selective serotonin reuptake inhibitors was not significant (adjusted hazard ratio 0.84, 95% confidence interval 0.47 to 1.50), but the suicide rate was significantly increased during periods of treatment with other antidepressants (2.64, 1.74 to 3.99). The hazard ratio for suicide was significantly increased for mirtazapine compared with citalopram (3.70, 2.00 to 6.84). Absolute risks of suicide over one year ranged from 0.02% for amitriptyline to 0.19% for mirtazapine. There was no significant difference in the rate of attempted suicide or self harm with tricyclic antidepressants (0.96, 0.87 to 1.08) compared with selective serotonin reuptake inhibitors, but the rate of attempted suicide or self harm was significantly higher for other antidepressants (1.80, 1.61 to 2.00). The adjusted hazard ratios for attempted suicide or self harm were significantly increased for three of the most commonly prescribed drugs compared with citalopram: venlafaxine (1.85, 1.61 to 2.13), trazodone (1.73, 1.26 to 2.37), and mirtazapine (1.70, 1.44 to 2.02), and significantly reduced for amitriptyline (0.71, 0.59 to 0.85). The absolute risks of attempted suicide or self harm over one year ranged from 1.02% for amitriptyline to 2.96% for venlafaxine. Rates were highest in the first 28 days after starting treatment and remained increased in the first 28 days after stopping treatment.
Conclusion: Rates of suicide and attempted suicide or self harm were similar during periods of treatment with selective serotonin reuptake inhibitors and tricyclic and related antidepressants. Mirtazapine, venlafaxine, and trazodone were associated with the highest rates of suicide and attempted suicide or self harm, but the number of suicide events was small leading to imprecise estimates. As this is an observational study the findings may reflect indication biases and residual confounding from severity of depression and differing characteristics of patients prescribed these drugs. The increased rates in the first 28 days of starting and stopping antidepressants emphasise the need for careful monitoring of patients during these periods.
© Coupland et al 2015.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures

Comment in
-
Antidepressants and risk of suicide.BMJ. 2015 Feb 19;350:h783. doi: 10.1136/bmj.h783. BMJ. 2015. PMID: 25698773 No abstract available.
-
Understanding the course of cognitive deficits over the onset of psychosis.Evid Based Ment Health. 2015 Aug;18(3):87. doi: 10.1136/eb-2014-101975. Epub 2015 May 4. Evid Based Ment Health. 2015. PMID: 25941270 Free PMC article. No abstract available.
-
Monitoring of suicide risk throughout the course of treatment with antidepressants for depression is required, but vigilance is required for those on some particular antidepressant agents.Evid Based Ment Health. 2015 Aug;18(3):86. doi: 10.1136/eb-2015-102102. Epub 2015 Jul 14. Evid Based Ment Health. 2015. PMID: 26173599 Free PMC article. No abstract available.
-
[Suicide risk varies by antidepressant].MMW Fortschr Med. 2015 Sep 24;157(16):41. doi: 10.1007/s15006-015-3537-9. MMW Fortschr Med. 2015. PMID: 26783623 German. No abstract available.
Similar articles
-
Antidepressant use and risk of adverse outcomes in older people: population based cohort study.BMJ. 2011 Aug 2;343:d4551. doi: 10.1136/bmj.d4551. BMJ. 2011. PMID: 21810886 Free PMC article.
-
A study of the safety and harms of antidepressant drugs for older people: a cohort study using a large primary care database.Health Technol Assess. 2011 Aug;15(28):1-202, iii-iv. doi: 10.3310/hta15280. Health Technol Assess. 2011. PMID: 21810375
-
Antidepressant use and risk of cardiovascular outcomes in people aged 20 to 64: cohort study using primary care database.BMJ. 2016 Mar 22;352:i1350. doi: 10.1136/bmj.i1350. BMJ. 2016. PMID: 27005565 Free PMC article.
-
Antidepressant drugs and the emergence of suicidal tendencies.Drug Saf. 1993 Mar;8(3):186-212. doi: 10.2165/00002018-199308030-00002. Drug Saf. 1993. PMID: 8452661 Review.
-
Antidepressants and suicidal risk.J Clin Psychiatry. 1999;60 Suppl 2:94-9; discussion 111-6. J Clin Psychiatry. 1999. PMID: 10073395 Review.
Cited by
-
Diabetes treatments and risk of heart failure, cardiovascular disease, and all cause mortality: cohort study in primary care.BMJ. 2016 Jul 12;354:i3477. doi: 10.1136/bmj.i3477. BMJ. 2016. PMID: 27413012 Free PMC article.
-
Reducing risk following self-harm: the need for careful prescribing.Br J Gen Pract. 2019 May;69(682):224-225. doi: 10.3399/bjgp19X702317. Br J Gen Pract. 2019. PMID: 31023669 Free PMC article. No abstract available.
-
Selective Serotonin Reuptake Inhibitor (SSRI) Antidepressants in Pregnancy and Congenital Anomalies: Analysis of Linked Databases in Wales, Norway and Funen, Denmark.PLoS One. 2016 Dec 1;11(12):e0165122. doi: 10.1371/journal.pone.0165122. eCollection 2016. PLoS One. 2016. PMID: 27906972 Free PMC article.
-
Antidepressants for pain management in adults with chronic pain: a network meta-analysis.Health Technol Assess. 2024 Oct;28(62):1-155. doi: 10.3310/MKRT2948. Health Technol Assess. 2024. PMID: 39367772 Free PMC article.
-
[Psychopharmaceuticals for treatment of suicidal patients and for suicide prevention].Nervenarzt. 2016 May;87(5):483-7. doi: 10.1007/s00115-016-0088-y. Nervenarzt. 2016. PMID: 26952239 Review. German.
References
-
- Harris EC, Barraclough B. Suicide as an outcome for mental disorders. A meta-analysis. Br J Psychiatry 1997;170:205-28. - PubMed
-
- Cassano P, Fava M. Depression and public health: an overview. J Psychosom Res 2002;53:849-57. - PubMed
-
- Friedman RA, Leon AC. Expanding the black box—depression, antidepressants, and the risk of suicide. N Engl J Med 2007;356:2343-6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials