

Multidisciplinary biopsychosocial rehabilitation for chronic low back pain: Cochrane systematic review and meta-analysis
- PMID: 25694111
- PMCID: PMC4353283
- DOI: 10.1136/bmj.h444
Multidisciplinary biopsychosocial rehabilitation for chronic low back pain: Cochrane systematic review and meta-analysis
Abstract
Objective: To assess the long term effects of multidisciplinary biopsychosocial rehabilitation for patients with chronic low back pain.
Design: Systematic review and random effects meta-analysis of randomised controlled trials.
Data sources: Electronic searches of Cochrane Back Review Group Trials Register, CENTRAL, Medline, Embase, PsycINFO, and CINAHL databases up to February 2014, supplemented by hand searching of reference lists and forward citation tracking of included trials.
Study selection criteria: Trials published in full; participants with low back pain for more than three months; multidisciplinary rehabilitation involved a physical component and one or both of a psychological component or a social or work targeted component; multidisciplinary rehabilitation was delivered by healthcare professionals from at least two different professional backgrounds; multidisciplinary rehabilitation was compared with a non- multidisciplinary intervention.
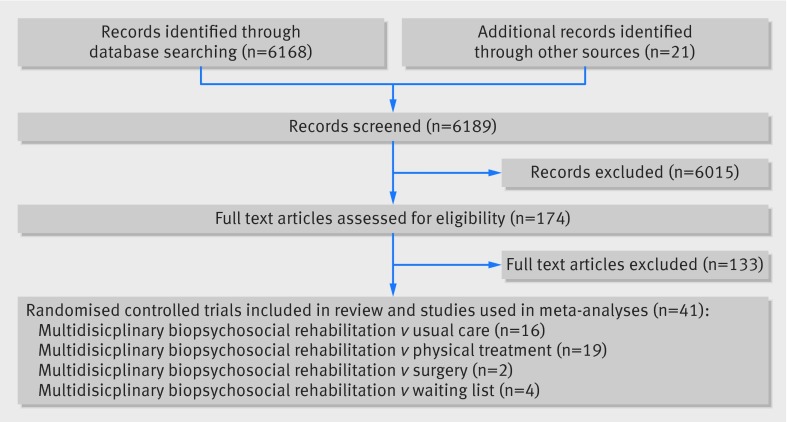
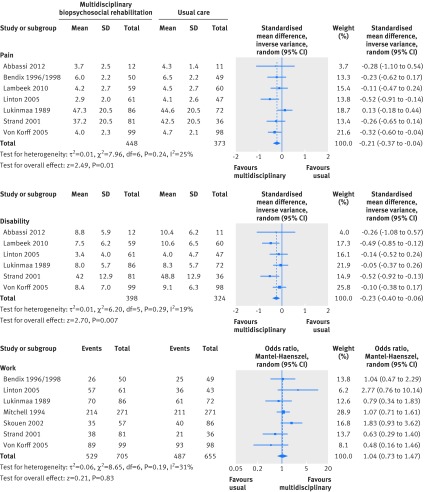
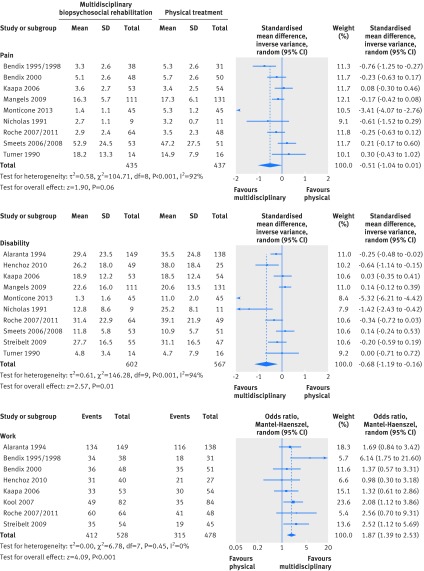
Results: Forty one trials included a total of 6858 participants with a mean duration of pain of more than one year who often had failed previous treatment. Sixteen trials provided moderate quality evidence that multidisciplinary rehabilitation decreased pain (standardised mean difference 0.21, 95% confidence interval 0.04 to 0.37; equivalent to 0.5 points in a 10 point pain scale) and disability (0.23, 0.06 to 0.40; equivalent to 1.5 points in a 24 point Roland-Morris index) compared with usual care. Nineteen trials provided low quality evidence that multidisciplinary rehabilitation decreased pain (standardised mean difference 0.51, -0.01 to 1.04) and disability (0.68, 0.16 to 1.19) compared with physical treatments, but significant statistical heterogeneity across trials was present. Eight trials provided moderate quality evidence that multidisciplinary rehabilitation improves the odds of being at work one year after intervention (odds ratio 1.87, 95% confidence interval 1.39 to 2.53) compared with physical treatments. Seven trials provided moderate quality evidence that multidisciplinary rehabilitation does not improve the odds of being at work (odds ratio 1.04, 0.73 to 1.47) compared with usual care. Two trials that compared multidisciplinary rehabilitation with surgery found little difference in outcomes and an increased risk of adverse events with surgery.
Conclusions: Multidisciplinary biopsychosocial rehabilitation interventions were more effective than usual care (moderate quality evidence) and physical treatments (low quality evidence) in decreasing pain and disability in people with chronic low back pain. For work outcomes, multidisciplinary rehabilitation seems to be more effective than physical treatment but not more effective than usual care.
© Kamper et al 2015.
Conflict of interest statement
Competing Interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Biopsychosocial care for chronic back pain.BMJ. 2015 Feb 18;350:h538. doi: 10.1136/bmj.h538. BMJ. 2015. PMID: 25693594 No abstract available.
-
Multidisciplinary biopsychosocial rehabilitation for chronic low back pain (PEDro synthesis).Br J Sports Med. 2016 Feb;50(4):251-2. doi: 10.1136/bjsports-2015-095413. Epub 2015 Sep 23. Br J Sports Med. 2016. PMID: 26400958 No abstract available.
-
Multidisciplinary Biopsychosocial Rehabilitation Improves Outcomes for Patients With Chronic Low Back Pain.J Am Osteopath Assoc. 2016 May 1;116(5):327-8. doi: 10.7556/jaoa.2016.068. J Am Osteopath Assoc. 2016. PMID: 27111791 No abstract available.
References
-
- Stanton TR, Latimer J, Maher CG, Hancock M. Definitions of recurrence of an episode of low back pain: a systematic review. Spine 2009;34:E316-22. - PubMed
-
- Lambeek LC, van Tulder MW, Swinkels IC, Koppes LL, Anema J, van Mechelen W. The trend in total cost of back pain in the Netherlands in the period 2002 to 2007. Spine 2011;36:1050-8. - PubMed
-
- Luo X, Pietrobon R, Sun SX, Liu GG, Hey L. Estimates and patterns of direct health care expenditures among individuals with back pain in the United States. Spine 2004;29:79-86. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical