

Preoperative Opioid Misuse is Associated With Increased Morbidity and Mortality After Elective Orthopaedic Surgery
- PMID: 25694266
- PMCID: PMC4457771
- DOI: 10.1007/s11999-015-4173-5
Preoperative Opioid Misuse is Associated With Increased Morbidity and Mortality After Elective Orthopaedic Surgery
Abstract
Background: Many patients having discretionary orthopaedic surgery take opioids daily, either with a prescription or illicitly, however little is known regarding the prevalence and effect of high-risk opioid use (eg, abuse, dependence) in the perioperative orthopaedic setting.
Questions/purposes: We sought (1) to determine the prevalence of opioid abuse and dependence in patients undergoing major elective orthopaedic surgery; (2) to characterize the relationship of opioid abuse and dependence with in-hospital postoperative mortality and adverse events, failure to rescue, prolonged length of stay, and nonroutine disposition; and (3) to identify factors associated with high-risk opioid use.
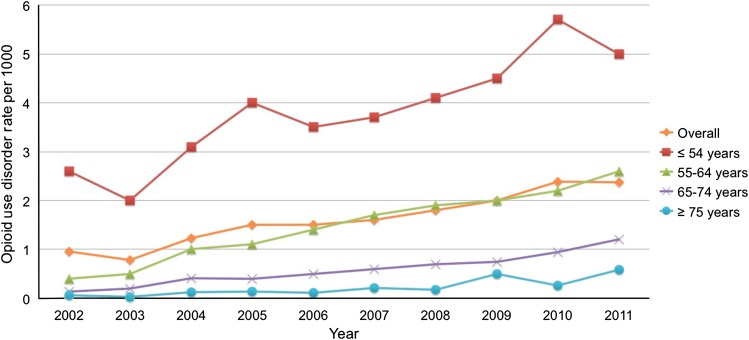
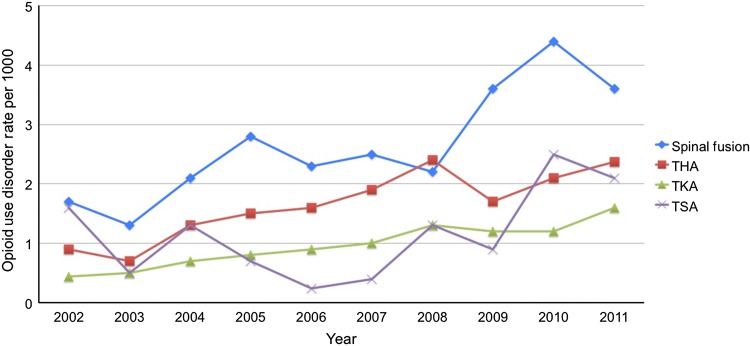
Methods: We used coding data collected in discharge records from the Nationwide Inpatient Sample (2002-2011). We analyzed changes with time in the prevalence of opioid abuse and dependence on admission. Finally, we used multivariate regression modeling to measure the association of opioid abuse and dependence with in-hospital postoperative mortality, morbidity, and resource utilization, and to identify factors associated with high-risk opioid use.
Results: The prevalence of opioid abuse and dependence increased from 0.095% in 2002 to 0.24% in 2011, an increase of 152% (p < 0.001). Opioid abuse and dependence were associated with increased inpatient mortality (odds ratio [OR], 3.7; 95% CI, 2.7-5.1) and aggregate morbidity (OR, 2.3 l; 95% CI, 2.2-2.4), including induced mental disorder (OR, 5.9; 95% CI, 5.4-6.3), respiratory failure (OR, 3.1; 95% CI, 2.7-3.6), surgical site infection (OR, 2.5; 95% CI, 2.0-3.0), mechanical ventilation (OR, 2.3; 95% CI, 2.0-2.5), pneumonia (OR, 2.1; 95% CI, 1.8-2.3), myocardial infarction (OR, 1.9; 95% CI, 1.3-2.6), and postoperative ileus or other gastrointestinal events (OR, 1.4; 95% CI, 1.3-1.6) (p < 0.001 for all listed entities). Abuse and dependence also were associated with increased risk for prolonged hospital length of stay (OR, 2.5; 95% CI, 2.4-2.5), nonroutine discharge (OR, 2.2; 95% CI, 2.2-2.3), and failure to rescue (OR, 2.0; 95% CI, 1.4-2.8). High-risk opioid users were more likely to be younger, male, nonwhite, Medicaid-insured patients with mental health and substance use disorders, and to be undergoing spine surgery. Hospital-related characteristics included urban setting, geographic location in the Northeast or West, and serving as a teaching facility.
Conclusion: Opioid abuse and dependence are increasing rapidly among orthopaedic surgical inpatients and are associated with considerable postoperative morbidity and mortality and resource utilization. We recommend that orthopaedic surgeons screen patients carefully for opioid misuse preoperatively, help patients who are using opioids inappropriately to discontinue them before scheduling elective surgery, decline to perform elective surgery in patients who misuse opioids, and closely monitor patients who are habituated to opioids at the time they undergo surgery.
Level of evidence: Level III, prognostic study.
Figures
Comment in
-
CORR Insights(®): Preoperative Opioid Misuse is Associated With Increased Morbidity and Mortality After Elective Orthopaedic Surgery.Clin Orthop Relat Res. 2015 Jul;473(7):2413-4. doi: 10.1007/s11999-015-4243-8. Epub 2015 Mar 10. Clin Orthop Relat Res. 2015. PMID: 25754759 Free PMC article. No abstract available.
References
-
- Altice FL, Bruce RD, Lucas GM, Lum PJ, Korthuis PT, Flanigan TP, Cunningham CO, Sullivan LE, Vergara-Rodriguez P, Fiellin DA, Cajina A, Botsko M, Nandi V, Gourevitch MN, Finkelstein R, BHIVES Collaborative HIV treatment outcomes among HIV-infected, opioid-dependent patients receiving buprenorphine/naloxone treatment within HIV clinical care settings: results from a multisite study. J Acquir Immune Defic Syndr. 2011;56(suppl 1):S22–32. doi: 10.1097/QAI.0b013e318209751e. - DOI - PMC - PubMed
-
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders-Dsm-5. 5. Washington, DC: American Psychiatric Association; 2013.
-
- Armaghani SJ, Lee DS, Bible JE, Archer KR, Shau DN, Kay H, Zhang C, McGirt MJ, Devin CJ. Preoperative narcotic use and its relation to depression and anxiety in patients undergoing spine surgery. Spine (Phila Pa 1976). 2013;38:2196–2000. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
