

Identification of chronic rhinosinusitis phenotypes using cluster analysis
- PMID: 25694390
- PMCID: PMC4428937
- DOI: 10.1002/alr.21496
Identification of chronic rhinosinusitis phenotypes using cluster analysis
Erratum in
-
Erratum.Int Forum Allergy Rhinol. 2017 Jan;7(1):106. doi: 10.1002/alr.21853. Epub 2016 Sep 14. Int Forum Allergy Rhinol. 2017. PMID: 28061022 No abstract available.
Abstract
Background: Current clinical classifications of chronic rhinosinusitis (CRS) have been largely defined based upon preconceived notions of factors thought to be important, such as polyp or eosinophil status. Unfortunately, these classification systems have little correlation with symptom severity or treatment outcomes. Unsupervised clustering can be used to identify phenotypic subgroups of CRS patients, describe clinical differences in these clusters and define simple algorithms for classification.
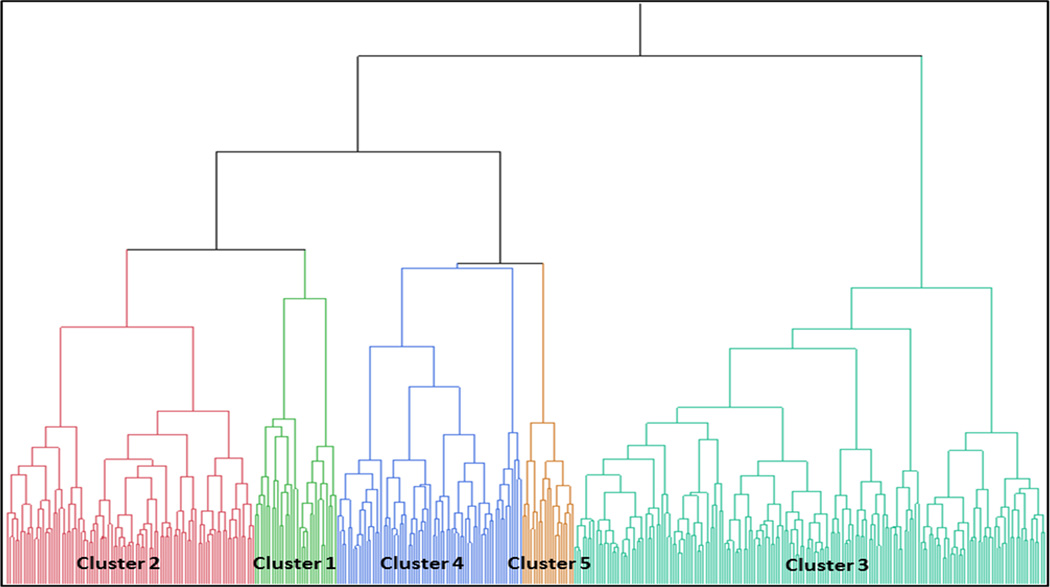
Methods: A multi-institutional, prospective study of 382 patients with CRS who had failed initial medical therapy completed the Sino-Nasal Outcome Test (SNOT-22), Rhinosinusitis Disability Index (RSDI), Medical Outcomes Study Short Form-12 (SF-12), Pittsburgh Sleep Quality Index (PSQI), and Patient Health Questionnaire (PHQ-2). Objective measures of CRS severity included Brief Smell Identification Test (B-SIT), CT, and endoscopy scoring. All variables were reduced and unsupervised hierarchical clustering was performed. After clusters were defined, variations in medication usage were analyzed. Discriminant analysis was performed to develop a simplified, clinically useful algorithm for clustering.
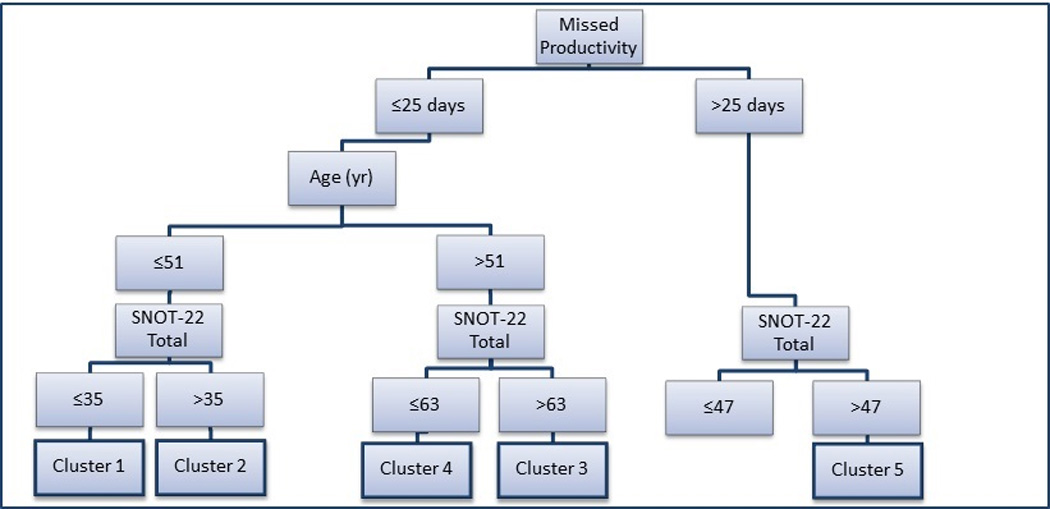
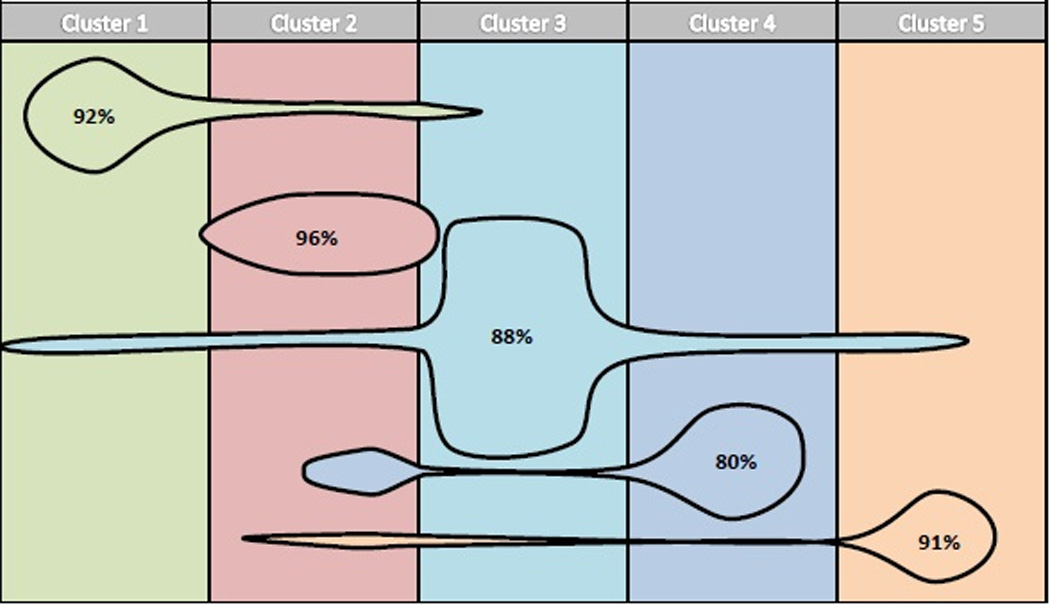
Results: Clustering was largely determined by age, severity of patient reported outcome measures, depression, and fibromyalgia. CT and endoscopy varied somewhat among clusters. Traditional clinical measures, including polyp/atopic status, prior surgery, B-SIT and asthma, did not vary among clusters. A simplified algorithm based upon productivity loss, SNOT-22 score, and age predicted clustering with 89% accuracy. Medication usage among clusters did vary significantly.
Conclusion: A simplified algorithm based upon hierarchical clustering is able to classify CRS patients and predict medication usage. Further studies are warranted to determine if such clustering predicts treatment outcomes.
Keywords: cluster analysis; phenotype; quality of life; sinusitis; staging.
© 2015 ARS-AAOA, LLC.
Conflict of interest statement
The authors have no other funding, financial relationships, or conflicts of interest to disclose.
Figures
References
-
- Fokkens WJ, Lund VJ, Mullol J, et al. EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinology. 2012;50:1–12. - PubMed
-
- Kountakis SE, Arango P, Bradley D, Wade ZK, Borish L. Molecular and cellular staging for the severity of chronic rhinosinusitis. The Laryngoscope. 2004;114:1895–1905. - PubMed
-
- Shi LL, Xiong P, Zhang L, et al. Features of airway remodeling in different types of Chinese chronic rhinosinusitis are associated with inflammation patterns. Allergy. 2013;68:101–109. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
