

A tool for prediction of risk of rehospitalisation and mortality in the hospitalised elderly: secondary analysis of clinical trial data
- PMID: 25694461
- PMCID: PMC4336459
- DOI: 10.1136/bmjopen-2014-007259
A tool for prediction of risk of rehospitalisation and mortality in the hospitalised elderly: secondary analysis of clinical trial data
Abstract
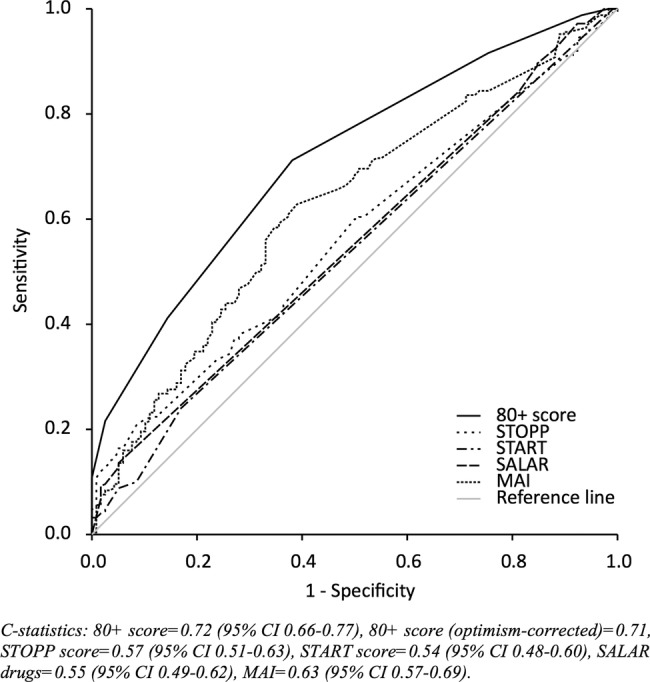
Objectives: To construct and internally validate a risk score, the '80+ score', for revisits to hospital and mortality for older patients, incorporating aspects of pharmacotherapy. Our secondary aim was to compare the discriminatory ability of the score with that of three validated tools for measuring inappropriate prescribing: Screening Tool of Older Person's Prescriptions (STOPP), Screening Tool to Alert doctors to Right Treatment (START) and Medication Appropriateness Index (MAI).
Setting: Two acute internal medicine wards at Uppsala University hospital. Patient data were used from a randomised controlled trial investigating the effects of a comprehensive clinical pharmacist intervention.
Participants: Data from 368 patients, aged 80 years and older, admitted to one of the study wards.
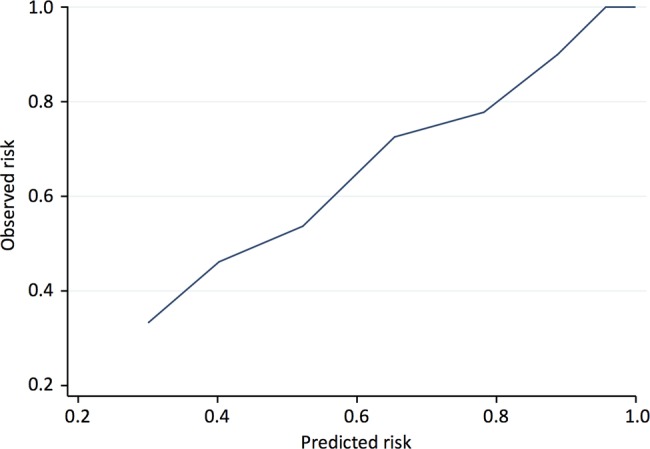
Primary outcome measure: Time to rehospitalisation or death during the year after discharge from hospital. Candidate variables were selected among a large number of clinical and drug-specific variables. After a selection process, a score for risk estimation was constructed. The 80+ score was internally validated, and the discriminatory ability of the score and of STOPP, START and MAI was assessed using C-statistics.
Results: Seven variables were selected. Impaired renal function, pulmonary disease, malignant disease, living in a nursing home, being prescribed an opioid or being prescribed a drug for peptic ulcer or gastroesophageal reflux disease were associated with an increased risk, while being prescribed an antidepressant drug (tricyclic antidepressants not included) was linked to a lower risk of the outcome. These variables made up the components of the 80+ score. The C-statistics were 0.71 (80+), 0.57 (STOPP), 0.54 (START) and 0.63 (MAI).
Conclusions: We developed and internally validated a score for prediction of risk of rehospitalisation and mortality in hospitalised older people. The score discriminated risk better than available tools for inappropriate prescribing. Pending external validation, this score can aid in clinical identification of high-risk patients and targeting of interventions.
Keywords: GERIATRIC MEDICINE; INTERNAL MEDICINE; Organisation of health services < HEALTH SERVICES ADMINISTRATION & MANAGEMENT; Prediction model; Risk-estimation; THERAPEUTICS (pharmacotherapy).
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical