

Statin-associated muscle symptoms: impact on statin therapy-European Atherosclerosis Society Consensus Panel Statement on Assessment, Aetiology and Management
- PMID: 25694464
- PMCID: PMC4416140
- DOI: 10.1093/eurheartj/ehv043
Statin-associated muscle symptoms: impact on statin therapy-European Atherosclerosis Society Consensus Panel Statement on Assessment, Aetiology and Management
Abstract
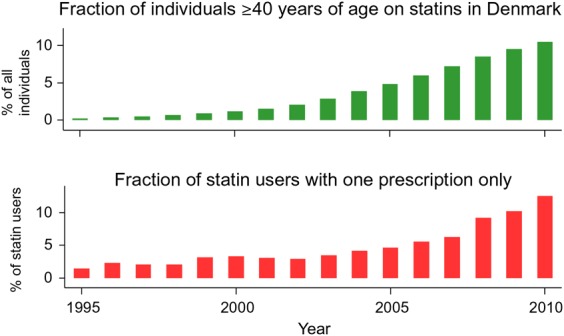
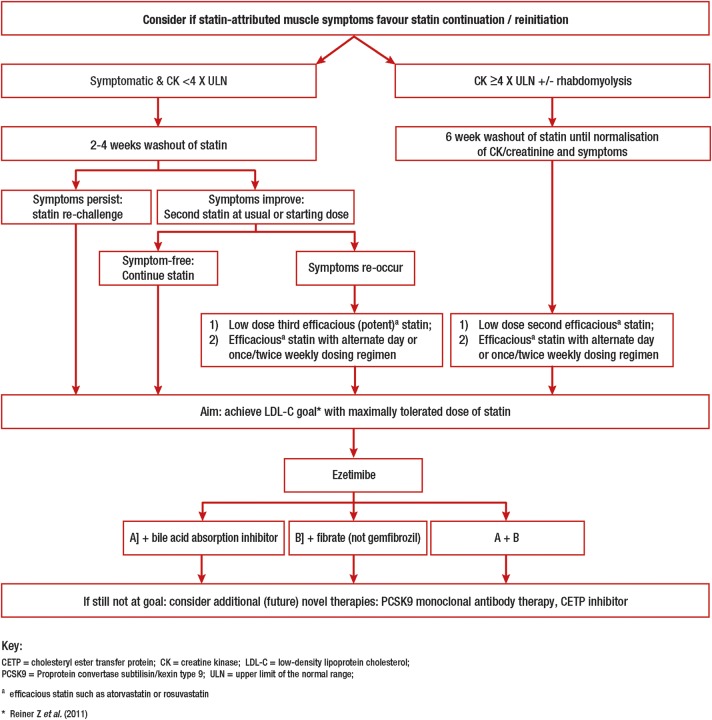
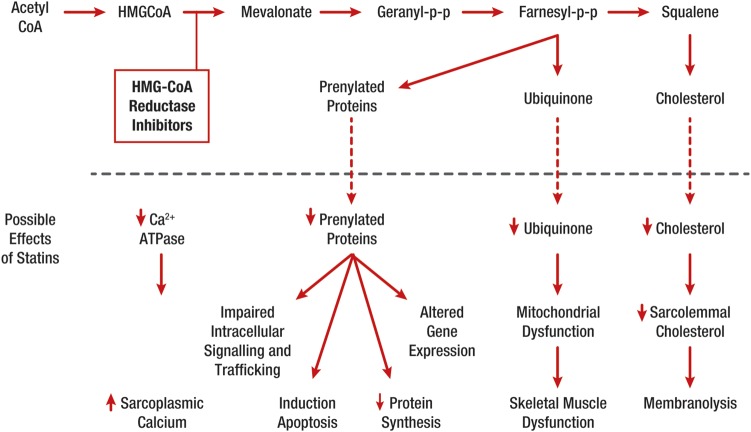
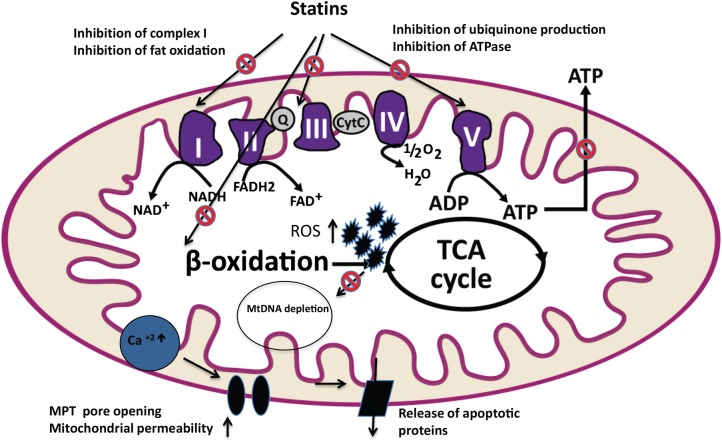
Statin-associated muscle symptoms (SAMS) are one of the principal reasons for statin non-adherence and/or discontinuation, contributing to adverse cardiovascular outcomes. This European Atherosclerosis Society (EAS) Consensus Panel overviews current understanding of the pathophysiology of statin-associated myopathy, and provides guidance for diagnosis and management of SAMS. Statin-associated myopathy, with significant elevation of serum creatine kinase (CK), is a rare but serious side effect of statins, affecting 1 per 1000 to 1 per 10 000 people on standard statin doses. Statin-associated muscle symptoms cover a broader range of clinical presentations, usually with normal or minimally elevated CK levels, with a prevalence of 7-29% in registries and observational studies. Preclinical studies show that statins decrease mitochondrial function, attenuate energy production, and alter muscle protein degradation, thereby providing a potential link between statins and muscle symptoms; controlled mechanistic and genetic studies in humans are necessary to further understanding. The Panel proposes to identify SAMS by symptoms typical of statin myalgia (i.e. muscle pain or aching) and their temporal association with discontinuation and response to repetitive statin re-challenge. In people with SAMS, the Panel recommends the use of a maximally tolerated statin dose combined with non-statin lipid-lowering therapies to attain recommended low-density lipoprotein cholesterol targets. The Panel recommends a structured work-up to identify individuals with clinically relevant SAMS generally to at least three different statins, so that they can be offered therapeutic regimens to satisfactorily address their cardiovascular risk. Further research into the underlying pathophysiological mechanisms may offer future therapeutic potential.
Keywords: Cholesterol; Consensus statement; Lipids; Mitochondrial; Muscle symptoms; Myalgia; Myopathy; Statin; Statin intolerance.
© The Author 2015. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Reiner Z, Catapano AL, De Backer G, Graham I, Taskinen MR, Wiklund O, Agewall S, Alegria E, Chapman MJ, Durrington P, Erdine S, Halcox J, Hobbs R, Kjekshus J, Filardi PP, Riccardi G, Storey RF, Wood D. ESC/EAS guidelines for the management of dyslipidaemias: the Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). Eur Heart J 2011;32:1769–1818. - PubMed
-
- Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet 2002;360:7–22.
-
- Ridker PM, Danielson E, Fonseca FA, Genest J, Gotto AM, Jr, Kastelein JJ, Koenig W, Libby P, Lorenzatti AJ, MacFadyen JG, Nordestgaard BG, Shepherd J, Willerson JT, Glynn RJ; JUPITER Study Group. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med 2008;359:2195–2207. - PubMed
-
- Kashani A, Phillips CO, Foody JM, Wang Y, Mangalmurti S, Ko DT, Krumholz HM. Risks associated with statin therapy: a systematic overview of randomized clinical trials. Circulation 2006;114:2788–2797. - PubMed
-
- Heart Outcomes Prevention Evaluation Study Investigators. Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: results of the HOPE study and MICRO-HOPE substudy. Lancet 2000;355:253–259. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
