

Endoscopic transforaminal decompression, interbody fusion, and percutaneous pedicle screw implantation of the lumbar spine: A case series report
- PMID: 25694885
- PMCID: PMC4300894
- DOI: 10.1016/j.ijsp.2012.04.001
Endoscopic transforaminal decompression, interbody fusion, and percutaneous pedicle screw implantation of the lumbar spine: A case series report
Abstract
Background: On the basis of the experiences gained from conventional open spinal procedures, a long list of desirable objectives have emerged with the evolution of the lesser invasive spinal procedures. At the top of that list is the desire to minimize the trauma of surgery. The rest of the objectives, which include reductions of operating time, surgical blood loss, hospital stay, postoperative narcotic medication, convalescence, complication rates, and escalating health care costs, as well as the desire of elderly patients to continue rigorous physical activities, largely depend on the ability to minimize the trauma of surgery. The purpose of this study was to investigate the feasibility of the least invasive lumbar decompression, interbody fusion and percutaneous pedicle screw implantation, to minimize surgical trauma without compromising the quality of the treatment outcome, as well as to minimize risk of complications.
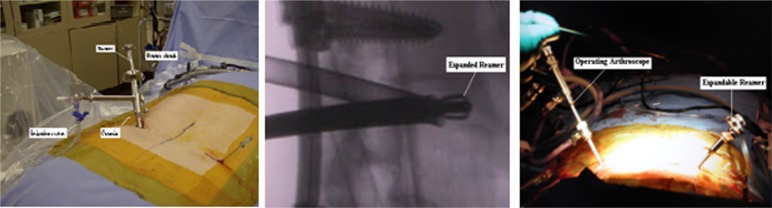
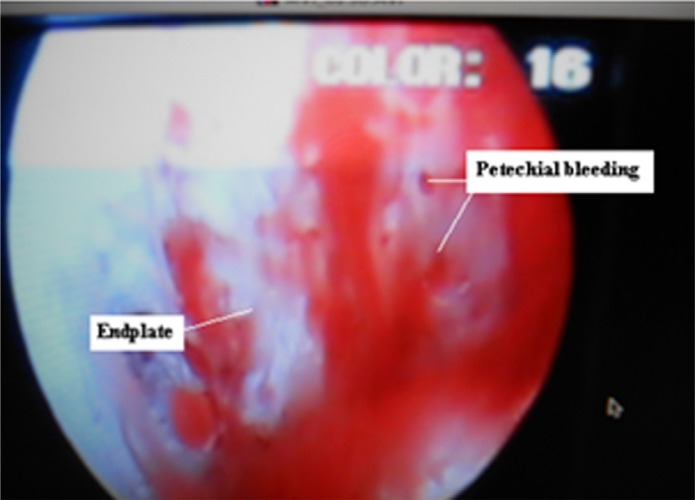
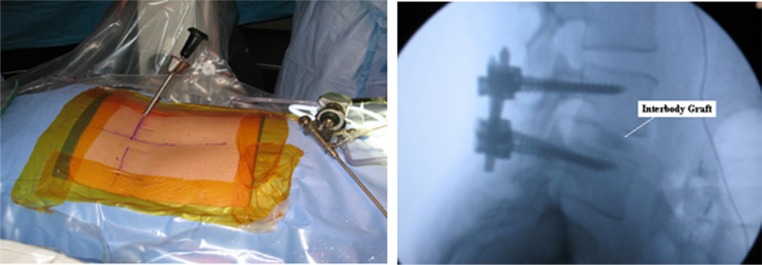
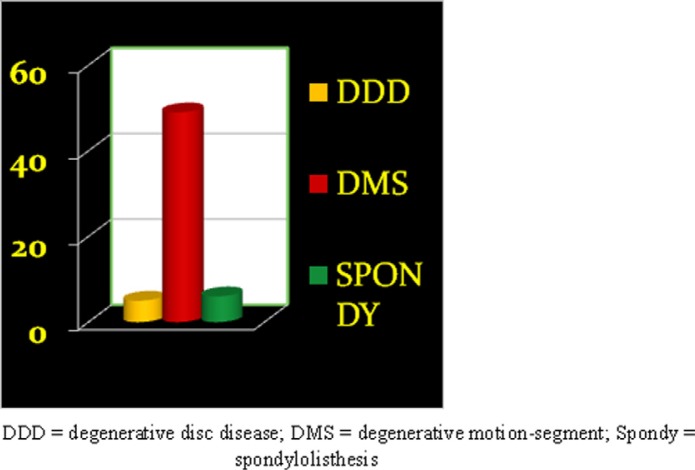
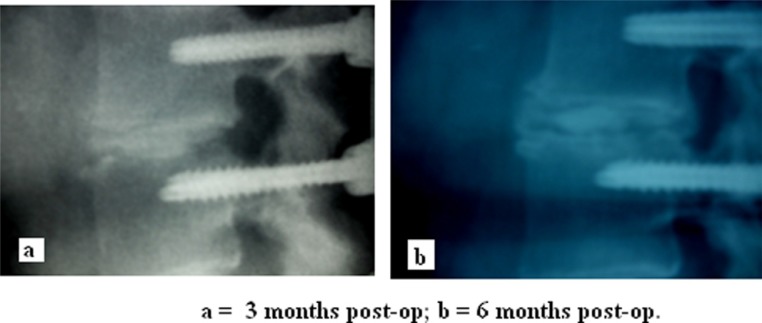
Methods: In this case series, 60 patients with diagnoses of degenerative disc disease, degenerative motion segments with stenosis, and spondylolisthesis, in whom nonoperative treatments failed, were treated with endoscopic transforaminal decompression and interbody fusion by 1 surgeon in 2 centers. The outcome measures were as follows: operating time, intraoperative blood loss, hospital stay, Visual Analogue Scale (VAS) scores for back and leg pain, scores on the Roland-Morris Disability Questionnaire, and postoperative imaging studies. A consecutive series of patients who met the treatment criteria completed VAS forms and Roland-Morris questionnaires preoperatively. Surgical procedures included arthroscopic decompression of the foramina and the discs; endplate preparation and implantation of allograft bone chips and bone morphogenetic protein 2 on absorbable collagen sponge into the disc space; and percutaneous implantation of pedicle screws. Postoperatively, the patients again completed the VAS forms and Roland-Morris questionnaires. Their charts were reviewed for office notes, operative notes, hospital stay, medications, and imaging studies. The latest X-ray and computed tomography scan films were reviewed and analyzed. Patients were followed up for a minimum of 6 months. The literature was reviewed for comparison of outcomes.
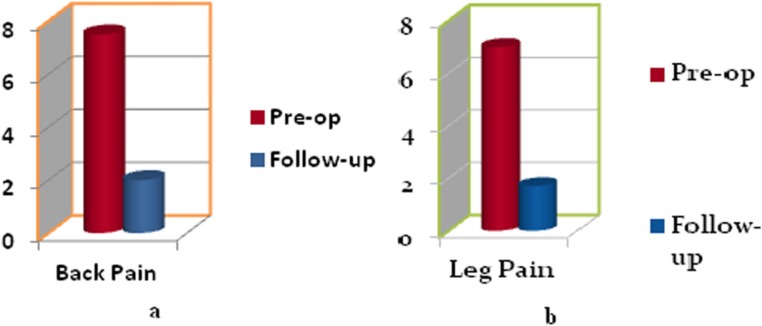
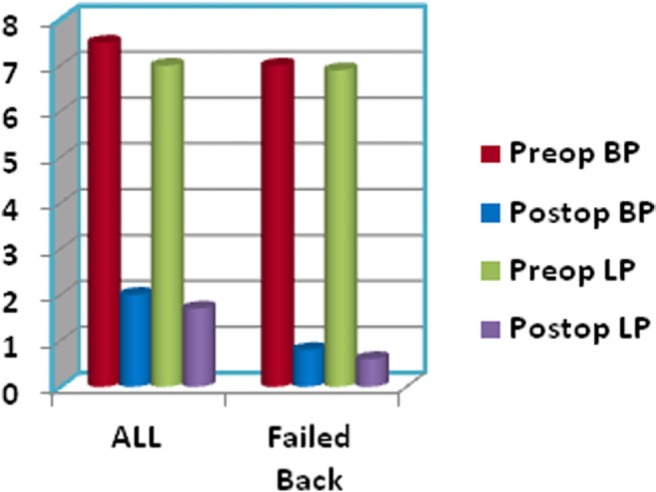
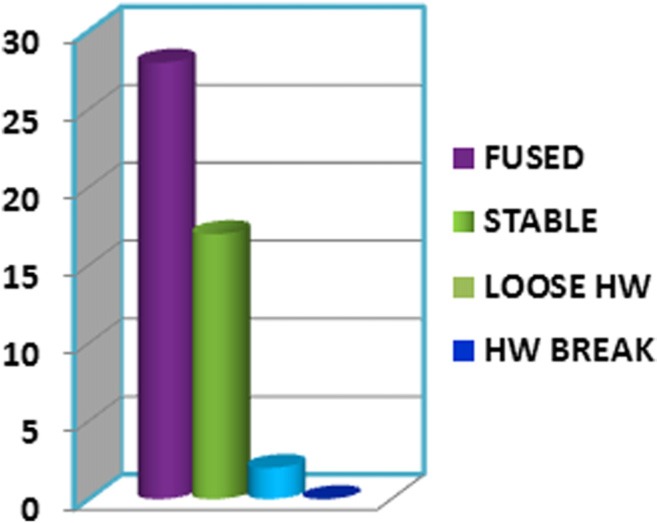
Results: Sixty patients met the inclusion criteria. The mean age was 52.8 years. The duration of illness averaged 5 years. Follow-up ranged from 6 to 25 months, with a mean of 12 months. Preoperative diagnoses included degenerative disc disease, degenerative motion segments with stenosis, and spondylolisthesis. The mean time in the operating room was 2 hours 54 minutes. Estimated blood loss averaged 57.6 mL. The duration of the hospital stay averaged 2.6 days. Preoperative back pain and leg pain were significantly reduced (P < .005). Forty-seven imaging studies obtained at the last visit, including X-ray and computed tomography scans, showed solid fusion in 28 patients (59.6%), stable fixation in 17 (36.2%), and osteolysis around the pedicle screws in 2 (4.2%). All patients had improvement of motor function, whereas 2 patients complained of residual numbness. In addition, 8 patients (13%) complained of residual discomfort on extension of the lumbar spine. Two patients had pedicle screw-related complications requiring surgery. A review of the literature showed that endoscopic transforaminal decompression and interbody fusion performed better than open transforaminal lumbar interbody fusion/posterior lumbar interbody fusion, minimally invasive transforaminal lumbar interbody fusion, and extreme lateral lumbar interbody fusion, with regard to most parameters studied.
Conclusions: The endoscopic transforaminal lumbar decompression, interbody fusion, and percutaneous pedicle screw instrumentation consistently produced satisfactory results in all demographics. It performed better than the alternative procedures for most parameters studied.
Keywords: Arthroscopic; BMP-2; ETDIF; Interbody; Percutaneous; Posterolateral.
Figures
References
-
- Deyo RA, Ciol MA, Cherkin DC, Loeser JD, Bigos SJ. Lumbar spinal fusion. A cohort study of complications, reoperations, and resource use in the Medicare population. Spine. 1993;18:1463–70. - PubMed
-
- Baker JK, Reardon PR, Reardon MJ, Heggeness MH. Vascular injury in anterior lumbar surgery. Spine. 1993;18:2227–30. - PubMed
-
- Rihn JA, Patel R, Makda J, et al. Complications associated with singlelevel transforaminal lumbar interbody fusion. Spine J. 2009;9:623–9. - PubMed
-
- Scaduto AA, Gamradt SC, Yu WD, Huang J, Delamarter RB, Wang JC. Perioperative complications of threaded cylindrical lumbar interbody fusion devices: Anterior versus posterior approach. J Spinal Disord Tech. 2003;16:502–7. - PubMed
-
- Kawaguchi Y, Matsui H, Tsuji H. Back muscle injury after posterior lumbar spine surgery. Part 1: Histologic and histochemical analyses in rats. Spine. 1994;19:2590–7. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous