

Ministernotomy or minithoracotomy for minimally invasive aortic valve replacement: a Bayesian network meta-analysis
- PMID: 25694971
- PMCID: PMC4311162
- DOI: 10.3978/j.issn.2225-319X.2014.08.01
Ministernotomy or minithoracotomy for minimally invasive aortic valve replacement: a Bayesian network meta-analysis
Abstract
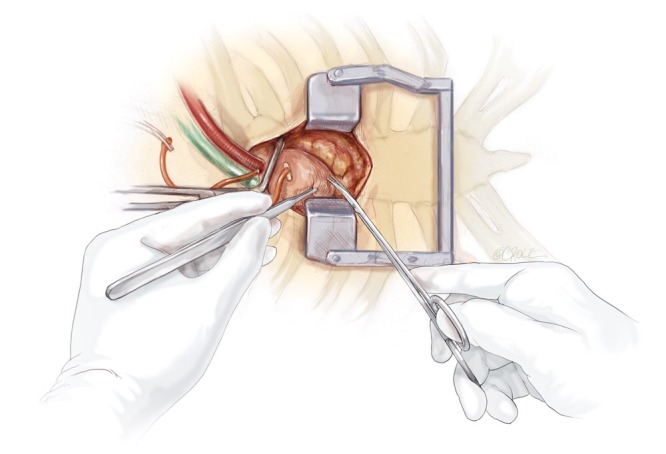
Background: Establishing the relative merits of ministernotomy (MS) and minithoracotomy (MT) approaches to minimally invasive aortic valve replacement (MIAVR) is difficult given the limited available direct evidence. Network meta-analysis is a Bayesian approach that can combine direct and indirect evidence to better define the benefits and risks of MS and MT.
Methods: Electronic searches were performed using six databases from their inception to June 2014. Relevant studies utilizing a minimally invasive approach for aortic valve replacement were identified. Data were extracted and analyzed according to predefined clinical endpoints. Both traditional and Bayesian meta-analysis approaches were conducted.
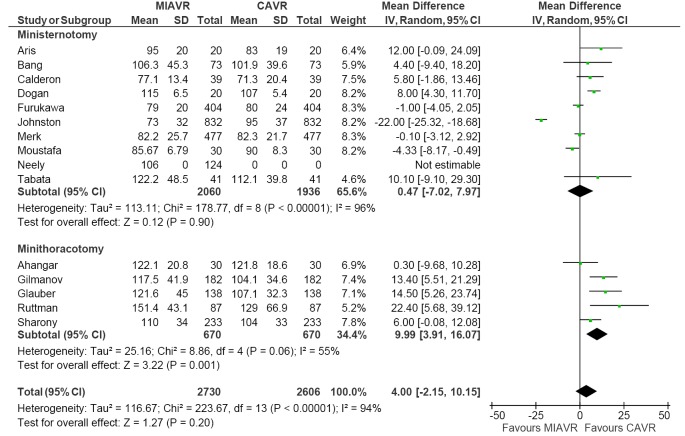
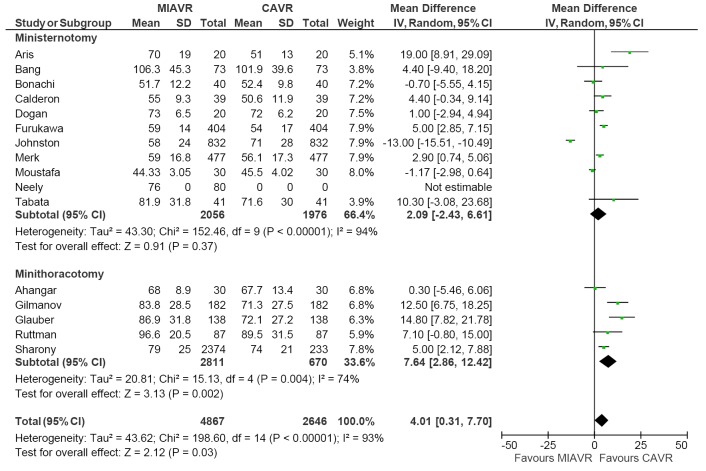
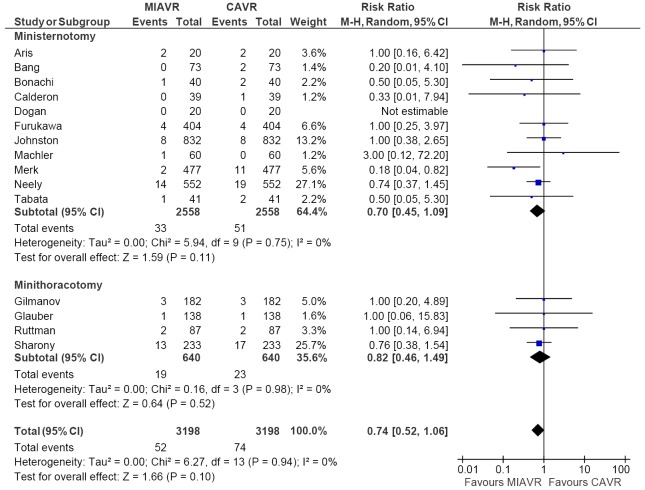
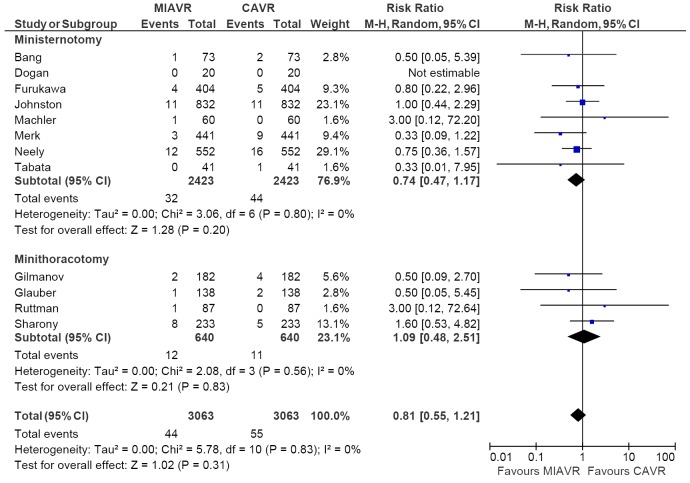
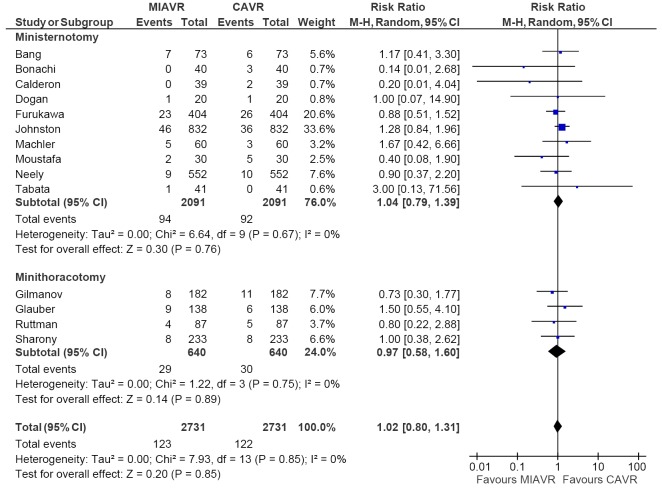
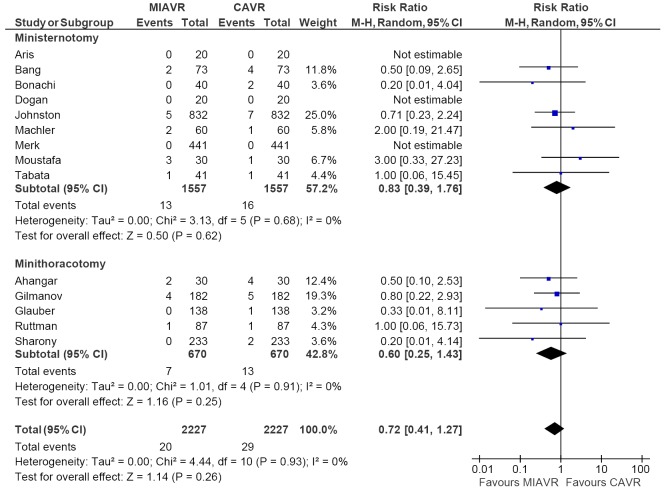
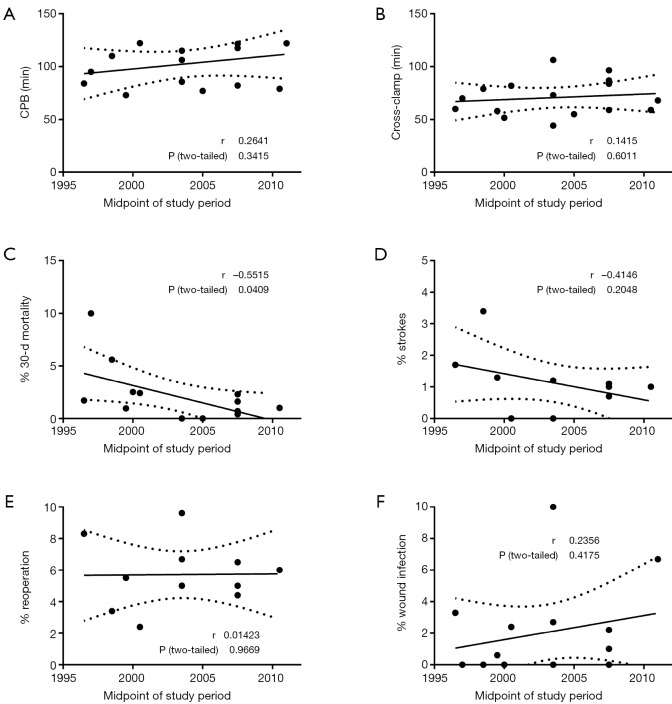
Results: Compared to full sternotomy, MT was associated with longer cardiopulmonary bypass (CPB) duration (WMD, 9.99; 95% CI, 3.91, 16.07; I(2)=55%; P=0.001) and cross-clamp duration (WMD, 7.64; 95% CI, 2.86, 12.42; P=0.002; I(2)=74%). When compared to MS using network meta-analysis, no significant difference in duration was detected. Postoperative outcomes including 30-day mortality, stroke, and reoperation for bleeding and wound infection were comparable between MS and MT using both traditional and Bayesian meta-analysis techniques.
Conclusions: The current evidence demonstrates that MIAVR via MS or MT is a safe and efficacious alternative to conventional median sternotomy. MT may be associated with longer CPB and cross-clamp durations, but has similar post-operative outcomes compared to MS. An individualized approach tailored to both the patient and surgical team is likely to provide optimal outcomes.
Keywords: Aortic valve replacement; Bayesian; ministernotomy; minithoracotomy; network meta-analysis.
Figures
References
-
- Murtuza B, Pepper JR, Stanbridge RD, et al. Minimal access aortic valve replacement: is it worth it? Ann Thorac Surg 2008;85:1121-31. - PubMed
-
- Phan K, Xie A, Di Eusanio M, et al. A Meta-Analysis of Minimally Invasive Versus Conventional Sternotomy for Aortic Valve Replacement. Ann Thorac Surg 2014;98:1499-511. - PubMed
-
- Glauber M, Miceli A, Bevilacqua S, et al. Minimally invasive aortic valve replacement via right anterior minithoracotomy: early outcomes and midterm follow-up. J Thorac Cardiovasc Surg 2011;142:1577-9. - PubMed
-
- Glauber M, Miceli A, Gilmanov D, et al. Right anterior minithoracotomy versus conventional aortic valve replacement: a propensity score matched study. J Thorac Cardiovasc Surg 2013;145:1222-6. - PubMed
-
- Glower DD, Desai BS, Hughes GC, et al. Aortic valve replacement via right minithoracotomy versus median sternotomy: a propensity score analysis. Innovations (Phila) 2014 ;9:75-81; discussion 81. - PubMed
Publication types
LinkOut - more resources
Full Text Sources