

Minimally invasive aortic valve replacement: the Leipzig experience
- PMID: 25694976
- PMCID: PMC4311153
- DOI: 10.3978/j.issn.2225-319X.2014.11.03
Minimally invasive aortic valve replacement: the Leipzig experience
Abstract
Background: Minimally invasive techniques are progressively challenging traditional approaches in cardiothoracic surgery. Minimally invasive aortic valve replacement (AVR) has become a routine procedure at our institution.
Methods: We retrospectively analyzed all patients undergoing minimally invasive isolated AVR between January 2003 and March 2014, at our institution. Mean follow-up was 4.7±4.3 years (range: 0-18 years) and was 99.8% complete.
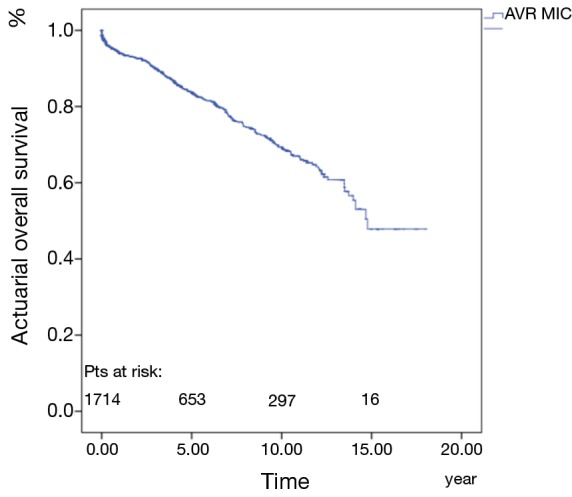
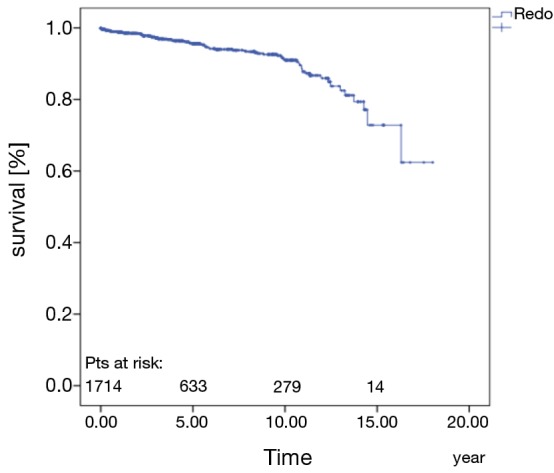
Results: There were 1,714 patients who received an isolated minimally invasive AVR. The mean (± SD) patient age was 65±12.8 years, ejection fraction 60%±12% and log EuroSCORE 5.3%±5.1%. Mean cross-clamp time was 58±18 minutes and mean cardiopulmonary bypass (CPB) time was 82.9±26.7 minutes. Thirty-day survival was 97.8%±0.4%, and 69.4%±1.7% at 10-years. The multivariate analysis revealed age at surgery [P=0.016; odds ratio (OR), 1.1], length of surgery time (P=0.002; OR, 1.01), female gender (P=0.023; OR, 3.54), preoperative myocardial infarction (MI) (P=0.006; OR, 7.87), preoperative stroke (P=0.001; OR, 13.76) and preoperative liver failure (P=0.015; OR, 10.28) as independent risk factors for mortality. Cox-regression analysis revealed the following predictors for long term mortality: age over 75 years (P<0.001; OR, 3.5), preoperative dialysis (P<0.01; OR, 2.14), ejection fraction less than 30% (P=0.003; OR, 3.28) and urgent or emergency operation (P<0.001; OR, 2.3).
Conclusions: Minimally invasive AVR can be performed safely and effectively with very few perioperative complications. The early and long-term outcomes in these patients are acceptable.
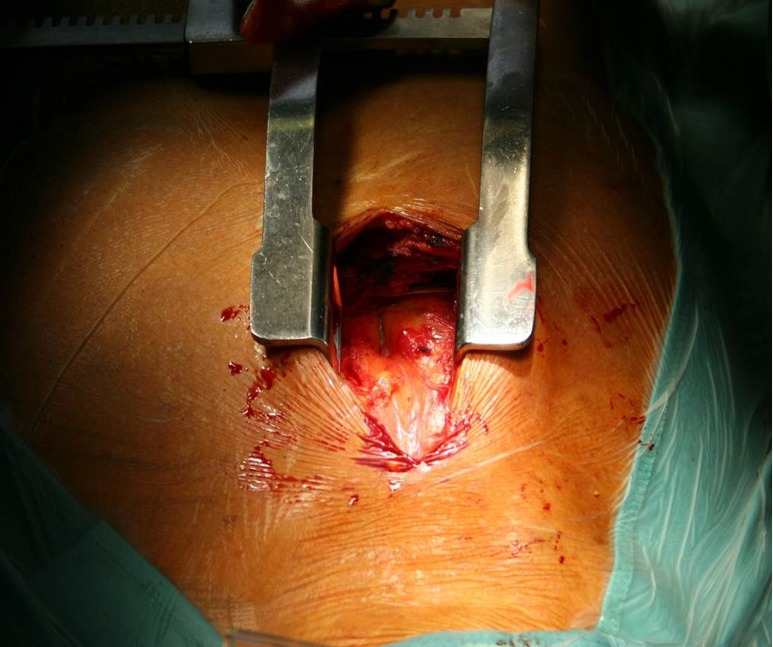
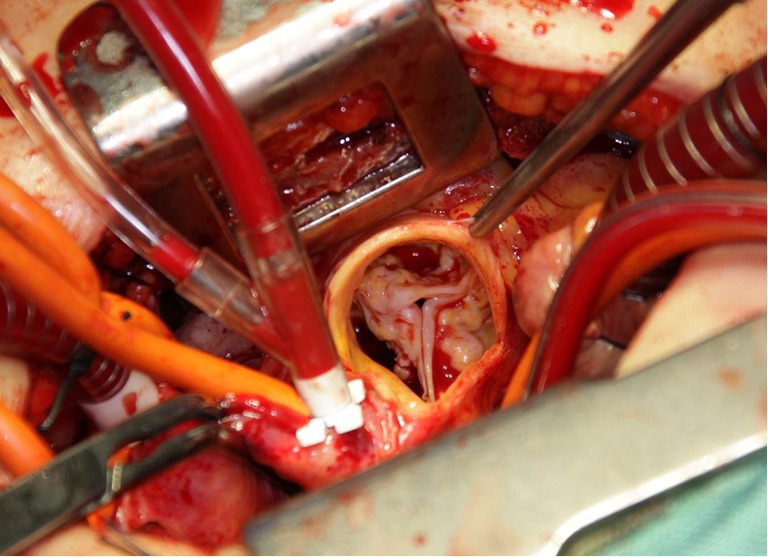
Keywords: Minimal invasive; aortic valve replacement (AVR); long-term survival; short-term survival; surgical technique.
Figures
Similar articles
-
Reoperative aortic valve replacement in the octogenarians-minimally invasive technique in the era of transcatheter valve replacement.J Thorac Cardiovasc Surg. 2014 Jan;147(1):155-62. doi: 10.1016/j.jtcvs.2013.08.076. Epub 2013 Nov 1. J Thorac Cardiovasc Surg. 2014. PMID: 24183906
-
Minimal invasive aortic valve replacement surgery is associated with improved survival: a propensity-matched comparison.Eur J Cardiothorac Surg. 2015 Jan;47(1):11-7; discussion 17. doi: 10.1093/ejcts/ezu068. Epub 2014 Mar 5. Eur J Cardiothorac Surg. 2015. PMID: 24599160
-
Predictive factors of long-term survival in the octogenarian undergoing surgical aortic valve replacement: 12-year single-centre follow-up.Heart Vessels. 2016 Nov;31(11):1798-1805. doi: 10.1007/s00380-016-0804-3. Epub 2016 Feb 3. Heart Vessels. 2016. PMID: 26843194
-
Minimally invasive aortic valve replacement versus aortic valve replacement through full sternotomy: the Brigham and Women's Hospital experience.Ann Cardiothorac Surg. 2015 Jan;4(1):38-48. doi: 10.3978/j.issn.2225-319X.2014.08.13. Ann Cardiothorac Surg. 2015. PMID: 25694975 Free PMC article.
-
Sutureless aortic valve replacement: a systematic review and meta-analysis.Ann Cardiothorac Surg. 2015 Mar;4(2):100-11. doi: 10.3978/j.issn.2225-319X.2014.06.01. Ann Cardiothorac Surg. 2015. PMID: 25870805 Free PMC article. Review.
Cited by
-
Minimally invasive aortic valve surgery.J Geriatr Cardiol. 2016 Sep;13(6):499-503. doi: 10.11909/j.issn.1671-5411.2016.06.005. J Geriatr Cardiol. 2016. PMID: 27582764 Free PMC article.
-
Surgical Therapy of Infective Prosthesis Endocarditis following TAVI: A Single Center's Experience.Diagnostics (Basel). 2024 Jun 14;14(12):1259. doi: 10.3390/diagnostics14121259. Diagnostics (Basel). 2024. PMID: 38928674 Free PMC article.
-
Mini-sternotomy versus conventional sternotomy for aortic valve replacement: a randomised controlled trial.BMJ Open. 2021 Jan 29;11(1):e041398. doi: 10.1136/bmjopen-2020-041398. BMJ Open. 2021. PMID: 33514577 Free PMC article. Clinical Trial.
-
Propensity matched analysis of minimally invasive versus conventional isolated aortic valve replacement.Perfusion. 2023 Mar;38(2):261-269. doi: 10.1177/02676591211045802. Epub 2021 Sep 13. Perfusion. 2023. PMID: 34515578 Free PMC article.
References
-
- Cosgrove DM, 3rd, Sabik JF. Minimally invasive approach for aortic valve operations. Ann Thorac Surg 1996;62:596-7. - PubMed
-
- Murtuza B, Pepper JR, Stanbridge RD, et al. Minimal access aortic valve replacement: is it worth it? Ann Thorac Surg 2008;85:1121-31. - PubMed
-
- Svensson LG, D’Agostino RS. “J” incision minimal-access valve operations. Ann Thorac Surg 1998;66:1110-2. - PubMed
-
- Farhat F, Lu Z, Lefevre M, et al. Prospective comparison between total sternotomy and ministernotomy for aortic valve replacement. J Card Surg 2003;18:396-401; discussion 402-3. - PubMed
-
- Glauber M, Miceli A, Gilmanov D, et al. Right anterior minithoracotomy versus conventional aortic valve replacement: a propensity score matched study. J Thorac Cardiovasc Surg 2013;145:1222-6. - PubMed
LinkOut - more resources
Full Text Sources