

Effectiveness of traveller screening for emerging pathogens is shaped by epidemiology and natural history of infection
- PMID: 25695520
- PMCID: PMC4337724
- DOI: 10.7554/eLife.05564
Effectiveness of traveller screening for emerging pathogens is shaped by epidemiology and natural history of infection
Abstract
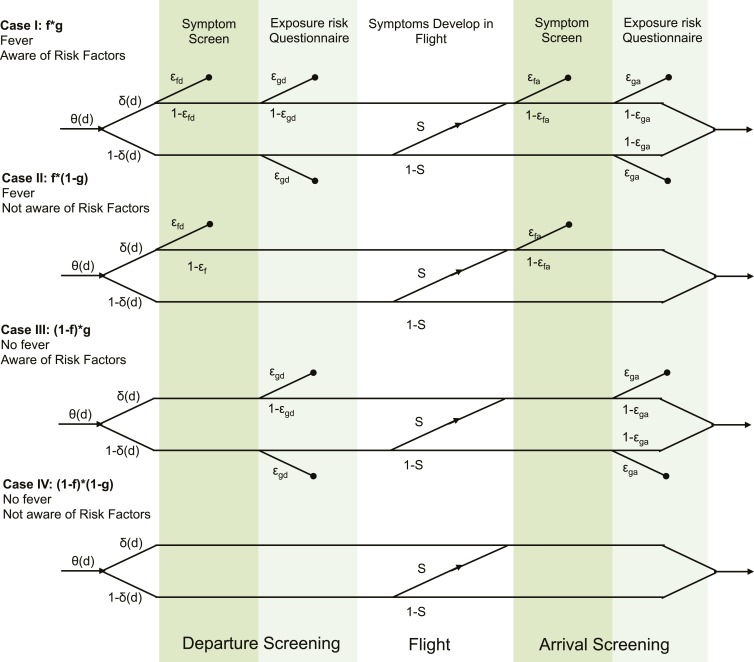
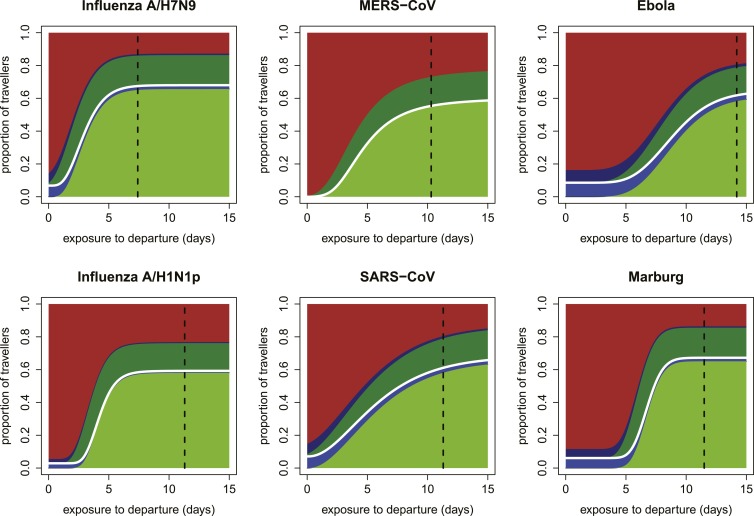
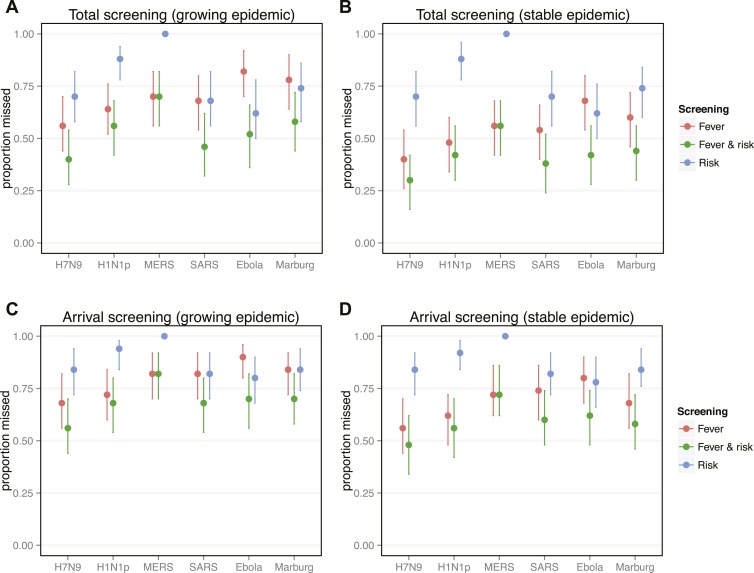
During outbreaks of high-consequence pathogens, airport screening programs have been deployed to curtail geographic spread of infection. The effectiveness of screening depends on several factors, including pathogen natural history and epidemiology, human behavior, and characteristics of the source epidemic. We developed a mathematical model to understand how these factors combine to influence screening outcomes. We analyzed screening programs for six emerging pathogens in the early and late stages of an epidemic. We show that the effectiveness of different screening tools depends strongly on pathogen natural history and epidemiological features, as well as human factors in implementation and compliance. For pathogens with longer incubation periods, exposure risk detection dominates in growing epidemics, while fever becomes a better target in stable or declining epidemics. For pathogens with short incubation, fever screening drives detection in any epidemic stage. However, even in the most optimistic scenario arrival screening will miss the majority of cases.
Keywords: ecology; emerging diseases; entry screening; epidemiology; fever screening; global health; incubation period; pathogen natural history; viruses.
Conflict of interest statement
The authors declare that no competing interests exist.
Figures






References
-
- Anderson RM, Fraser C, Ghani AC, Donnelly CA, Riley S, Ferguson NM, Leung GM, Lam TH, Hedley AJ. Epidemiology, transmission dynamics and control of SARS: the 2002-2003 epidemic. Philosophical Transactions of the Royal Society B: Biological Sciences. 2004;359:1091–1105. doi: 10.1098/rstb.2004.1490. - DOI - PMC - PubMed
-
- Apuzzo M, Fernandez M. 5 U.S. Airports set for travelers from 3 west African Nations. New York Times 2014
-
- Assiri A, McGeer A, Perl TM, Price CS, Al Rabeeah AA, Cummings DA, Alabdullatif ZN, Assad M, Almulhim A, Makhdoom H, Madani H, Alhakeem R, Al-Tawfiq JA, Cotten M, Watson SJ, Kellam P, Zumla AI, Memish ZA, KSA MERS-CoV Investigation Team Hospital outbreak of Middle East respiratory syndrome coronavirus. New England Journal of Medicine. 2013;369:407–416. doi: 10.1056/NEJMoa1306742. - DOI - PMC - PubMed
