

Human trachealis and main bronchi smooth muscle are normoresponsive in asthma
- PMID: 25695616
- PMCID: PMC4435453
- DOI: 10.1164/rccm.201407-1296OC
Human trachealis and main bronchi smooth muscle are normoresponsive in asthma
Abstract
Rationale: Airway smooth muscle (ASM) plays a key role in airway hyperresponsiveness (AHR) but it is unclear whether its contractility is intrinsically changed in asthma.
Objectives: To investigate whether key parameters of ASM contractility are altered in subjects with asthma.
Methods: Human trachea and main bronchi were dissected free of epithelium and connective tissues and suspended in a force-length measurement set-up. After equilibration each tissue underwent a series of protocols to assess its methacholine dose-response relationship, shortening velocity, and response to length oscillations equivalent to tidal breathing and deep inspirations.
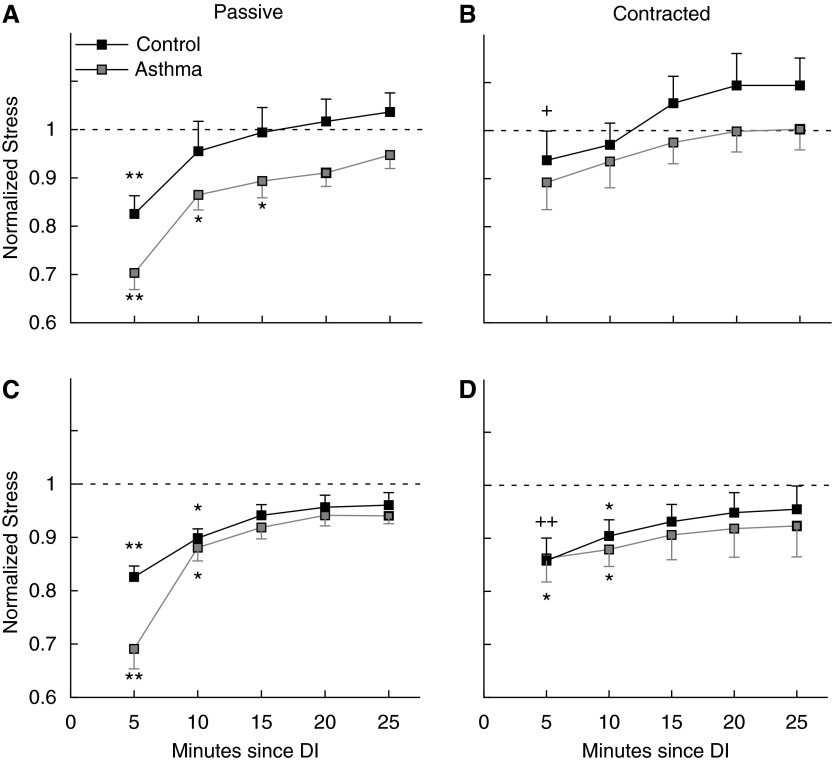
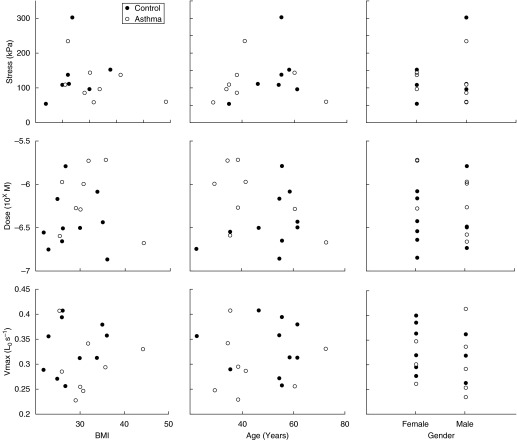
Measurements and main results: Main bronchi and tracheal ASM were significantly hyposensitive in subjects with asthma compared with control subjects. Trachea and main bronchi did not show significant differences in reactivity to methacholine and unloaded tissue shortening velocity (Vmax) compared with control subjects. There were no significant differences in responses to deep inspiration, with or without superimposed tidal breathing oscillations. No significant correlations were found between age, body mass index, or sex and sensitivity, reactivity, or Vmax.
Conclusions: Our data show that, in contrast to some animal models of AHR, human tracheal and main bronchial smooth muscle contractility is not increased in asthma. Specifically, our results indicate that it is highly unlikely that ASM half-maximum effective concentration (EC50) or Vmax contribute to AHR in asthma, but, because of high variability, we cannot conclude whether or not asthmatic ASM is hyperreactive.
Keywords: airway hyperresponsiveness; airway smooth muscle mechanics; asthma; shortening velocity; smooth muscle.
Figures



References
-
- Cockcroft DW, Killian DN, Mellon JJ, Hargreave FE. Bronchial reactivity to inhaled histamine: a method and clinical survey. Clin Allergy. 1977;7:235–243. - PubMed
-
- Bai TR. Abnormalities in airway smooth muscle in fatal asthma: a comparison between trachea and bronchus. Am Rev Respir Dis. 1991;143:441–443. - PubMed
-
- Bai TR. Abnormalities in airway smooth muscle in fatal asthma. Am Rev Respir Dis. 1990;141:552–557. - PubMed
-
- de Jongste JC, van Strik R, Bonta IL, Kerrebijn KF. Measurement of human small airway smooth muscle function in vitro with the bronchiolar strip preparation. J Pharmacol Methods. 1985;14:111–118. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
