

Association of hospital-level volume of extracorporeal membrane oxygenation cases and mortality. Analysis of the extracorporeal life support organization registry
- PMID: 25695688
- PMCID: PMC4435456
- DOI: 10.1164/rccm.201409-1634OC
Association of hospital-level volume of extracorporeal membrane oxygenation cases and mortality. Analysis of the extracorporeal life support organization registry
Abstract
Rationale: Recent pediatric studies suggest a survival benefit exists for higher-volume extracorporeal membrane oxygenation (ECMO) centers.
Objectives: To determine if higher annual ECMO patient volume is associated with lower case-mix-adjusted hospital mortality rate.
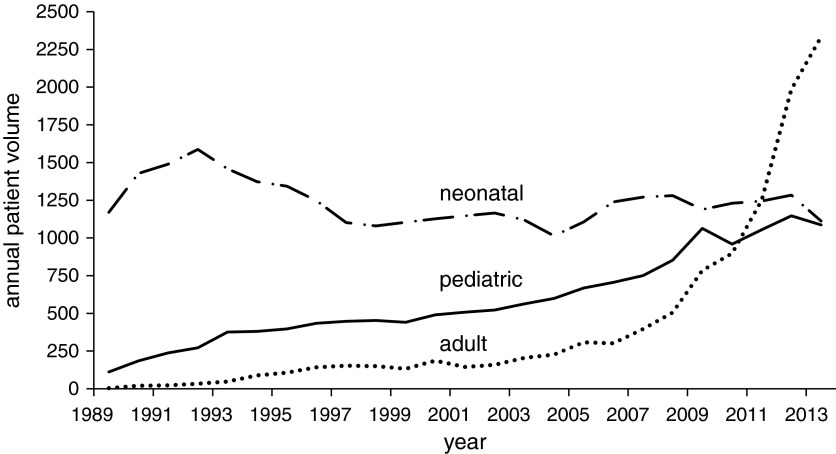
Methods: We retrospectively analyzed an international registry of ECMO support from 1989 to 2013. Patients were separated into three age groups: neonatal (0-28 d), pediatric (29 d to <18 yr), and adult (≥18 yr). The measure of hospital ECMO volume was age group-specific and adjusted for patient-level case-mix and hospital-level variance using multivariable hierarchical logistic regression modeling. The primary outcome was death before hospital discharge. A subgroup analysis was conducted for 2008-2013.
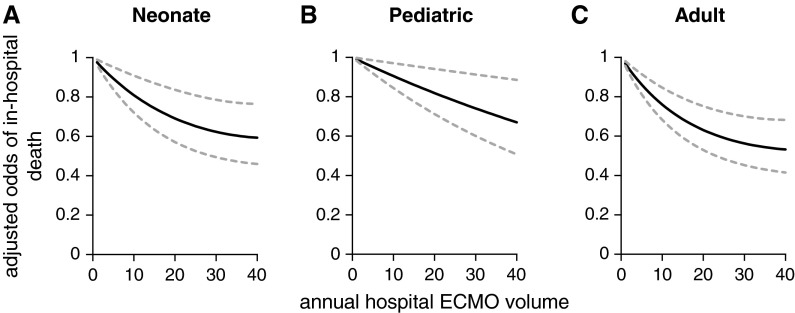
Measurements and main results: From 1989 to 2013, a total of 290 centers provided ECMO support to 56,222 patients (30,909 neonates, 14,725 children, and 10,588 adults). Annual ECMO mortality rates varied widely across ECMO centers: the interquartile range was 18-50% for neonates, 25-66% for pediatrics, and 33-92% for adults. For 1989-2013, higher age group-specific ECMO volume was associated with lower odds of ECMO mortality for neonates and adults but not for pediatric cases. In 2008-2013, the volume-outcome association remained statistically significant only among adults. Patients receiving ECMO at hospitals with more than 30 adult annual ECMO cases had significantly lower odds of mortality (adjusted odds ratio, 0.61; 95% confidence interval, 0.46-0.80) compared with adults receiving ECMO at hospitals with less than six annual cases.
Conclusions: In this international, case-mix-adjusted analysis, higher annual hospital ECMO volume was associated with lower mortality in 1989-2013 for neonates and adults; the association among adults persisted in 2008-2013.
Keywords: adult; extracorporeal membrane oxygenation; high-volume hospitals; low-volume hospitals; pediatric.
Figures
Comment in
-
Higher volumes, better outcomes: the end or just the beginning of the story for extracorporeal membrane oxygenation?Am J Respir Crit Care Med. 2015 Apr 15;191(8):864-6. doi: 10.1164/rccm.201503-0459ED. Am J Respir Crit Care Med. 2015. PMID: 25876197 No abstract available.
References
-
- Noah MA, Peek GJ, Finney SJ, Griffiths MJ, Harrison DA, Grieve R, Sadique MZ, Sekhon JS, McAuley DF, Firmin RK, et al. Referral to an extracorporeal membrane oxygenation center and mortality among patients with severe 2009 influenza A(H1N1) JAMA. 2011;306:1659–1668. - PubMed
-
- Brodie D, Bacchetta M. Extracorporeal membrane oxygenation for ARDS in adults. N Engl J Med. 2011;365:1905–1914. - PubMed
-
- UK Collaborative ECMO Trail Group. UK collaborative randomised trial of neonatal extracorporeal membrane oxygenation. Lancet. 1996;348:75–82. - PubMed
-
- Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, Thalanany MM, Hibbert CL, Truesdale A, Clemens F, Cooper N, et al. CESAR trial collaboration. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet. 2009;374:1351–1363. - PubMed
-
- Fraser CD, Jr, Jaquiss RD, Rosenthal DN, Humpl T, Canter CE, Blackstone EH, Naftel DC, Ichord RN, Bomgaars L, Tweddell JS, et al. Berlin Heart Study Investigators. Prospective trial of a pediatric ventricular assist device. N Engl J Med. 2012;367:532–541. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
