

MRI characteristics of neuromyelitis optica spectrum disorder: an international update
- PMID: 25695963
- PMCID: PMC4371410
- DOI: 10.1212/WNL.0000000000001367
MRI characteristics of neuromyelitis optica spectrum disorder: an international update
Abstract
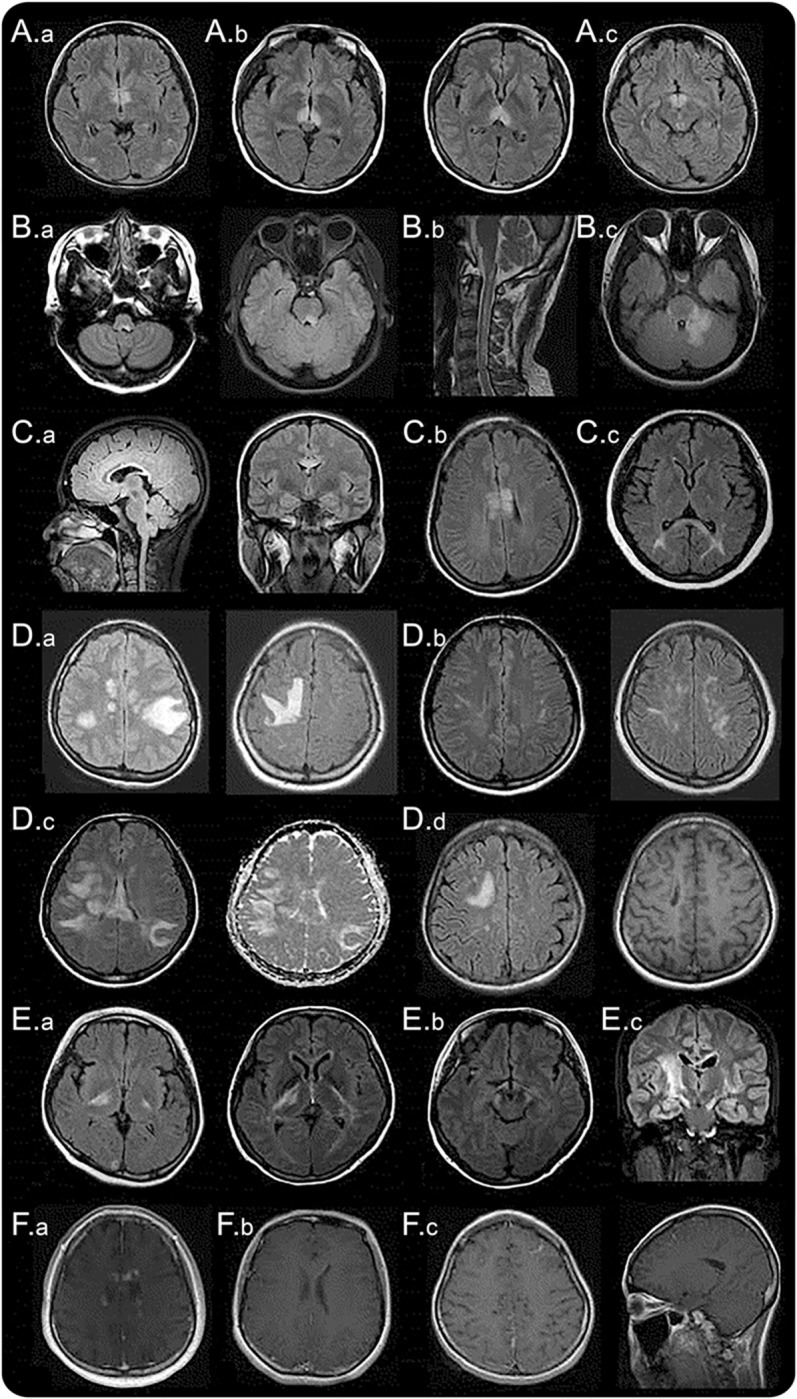
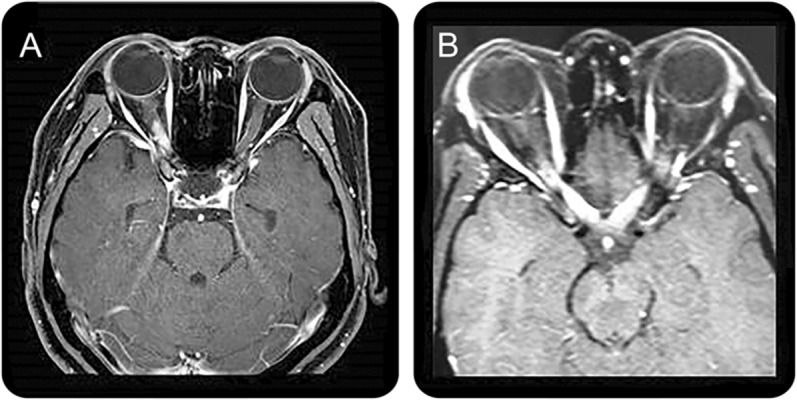
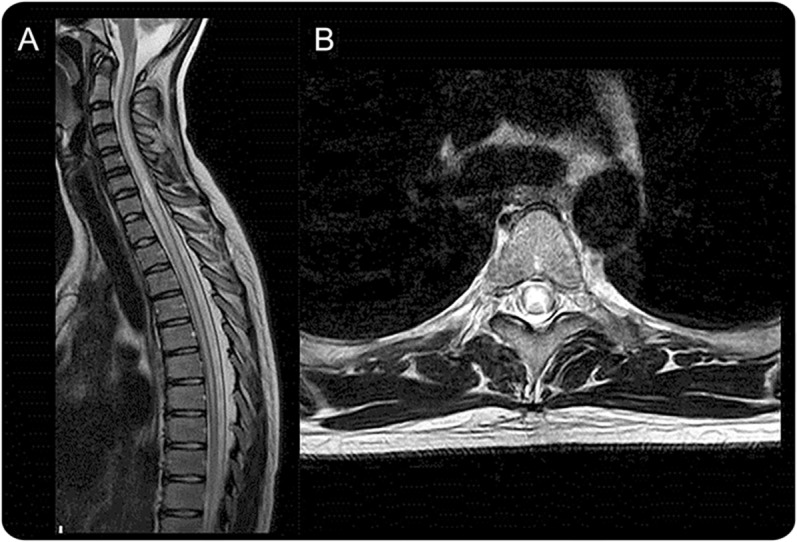
Since its initial reports in the 19th century, neuromyelitis optica (NMO) had been thought to involve only the optic nerves and spinal cord. However, the discovery of highly specific anti-aquaporin-4 antibody diagnostic biomarker for NMO enabled recognition of more diverse clinical spectrum of manifestations. Brain MRI abnormalities in patients seropositive for anti-aquaporin-4 antibody are common and some may be relatively unique by virtue of localization and configuration. Some seropositive patients present with brain involvement during their first attack and/or continue to relapse in the same location without optic nerve and spinal cord involvement. Thus, characteristics of brain abnormalities in such patients have become of increased interest. In this regard, MRI has an increasingly important role in the differential diagnosis of NMO and its spectrum disorder (NMOSD), particularly from multiple sclerosis. Differentiating these conditions is of prime importance because early initiation of effective immunosuppressive therapy is the key to preventing attack-related disability in NMOSD, whereas some disease-modifying drugs for multiple sclerosis may exacerbate the disease. Therefore, identifying the MRI features suggestive of NMOSD has diagnostic and prognostic implications. We herein review the brain, optic nerve, and spinal cord MRI findings of NMOSD.
© 2015 American Academy of Neurology.
Figures

References
-
- Wingerchuk DM, Hogancamp WF, O'Brien PC, Weinshenker BG. The clinical course of neuromyelitis optica (Devic's syndrome). Neurology 1999;53:1107–1114. - PubMed
-
- Lennon VA, Wingerchuk DM, Kryzer TJ, et al. A serum autoantibody marker of neuromyelitis optica: distinction from multiple sclerosis. Lancet 2004;364:2106–2112. - PubMed
-
- Wingerchuk DM, Lennon VA, Pittock SJ, Lucchinetti CF, Weinshenker BG. Revised diagnostic criteria for neuromyelitis optica. Neurology 2006;66:1485–1489. - PubMed
-
- Wingerchuk DM, Lennon VA, Lucchinetti CF, Pittock SJ, Weinshenker BG. The spectrum of neuromyelitis optica. Lancet Neurol 2007;6:805–815. - PubMed
-
- Kim SH, Kim W, Li XF, Jung IJ, Kim HJ. Clinical spectrum of CNS aquaporin-4 autoimmunity. Neurology 2012;78:1179–1185. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical