

The impact of trauma-center care on mortality and function following pelvic ring and acetabular injuries
- PMID: 25695975
- PMCID: PMC6948797
- DOI: 10.2106/JBJS.N.00008
The impact of trauma-center care on mortality and function following pelvic ring and acetabular injuries
Abstract
Background: Lower mortality and improved physical function following major polytrauma have been associated with treatment at level-I trauma centers compared with that at hospitals without a trauma center (nontrauma centers). This study investigated the impact of trauma-center care on outcomes after pelvic and acetabular injuries.
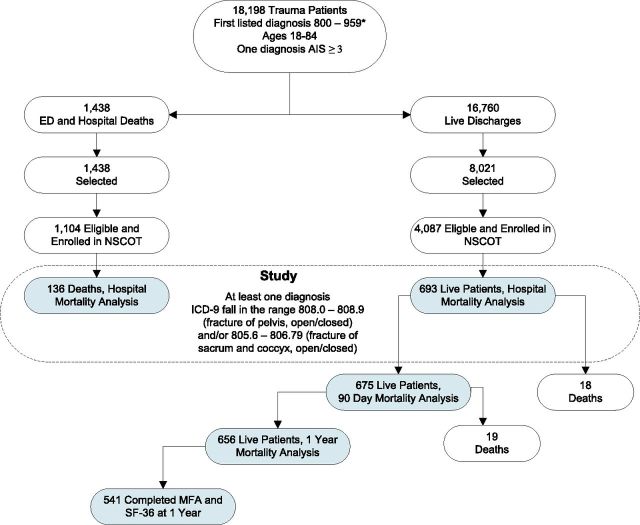
Methods: Mortality and quality-of-life-related scores were compared among patients treated in eighteen level-I trauma centers and fifty-one nontrauma centers in fourteen U.S. states. Complete data were obtained on 829 adult trauma patients (eighteen to eighty-four years old) who had at least one pelvic ring or acetabular injury (Orthopaedic Trauma Association [OTA] classification of 61 or 62). We used inverse probability of treatment weighting to adjust for observable confounding.
Results: After adjusting for case mix, we found that, for patients with more severe acetabular injuries (OTA 62-B or 62-C), in-hospital mortality was significantly lower at trauma centers compared with nontrauma centers (relative risk [RR], 0.10; 95% confidence interval [CI], 0.02 to 0.47), as was death within ninety days (RR, 0.10; 95% CI, 0.02 to 0.47) and within one year (RR, 0.21; 95% CI, 0.06 to 0.76). Patients with combined pelvic ring and acetabular injuries treated at a trauma center had lower mortality at ninety days (RR, 0.34; 95% CI, 0.14 to 0.82) and at one year (RR, 0.30; 95% CI, 0.14 to 0.68). Care at trauma centers was also associated with mortality risk reduction for those with unstable pelvic ring injuries (OTA 61-B or 61-C) at one year (RR, 0.71; 95% CI, 0.24 to 0.91). Seventy-eight percent of included subjects discharged alive were available for interview at twelve months. For those with more severe acetabular injuries, average absolute differences in the Short Form-36 (SF-36) physical function component and the Musculoskeletal Function Assessment at one year were 11.4 (95% CI, 5.3 to 17.4) and 13.2 (1.7 to 24.7), respectively, indicating statistically and clinically significant improved outcomes following treatment at a trauma center for those patients.
Conclusions: Mortality was reduced for patients with unstable pelvic and severe acetabular injuries when care was provided in a trauma center compared with a nontrauma center. Moreover, those with severe acetabular fractures experienced improved physical function at one year. Patients with these injuries represent a well-defined subset of trauma patients for whom our findings suggest preferential triage or transfer to a level-I trauma center.
Copyright © 2015 by The Journal of Bone and Joint Surgery, Incorporated.
Figures
Comment in
-
Caring for the critically injured. Commentary on an article by Saam Morshed, MD, PhD, MPH, et al.: "The impact of trauma-center care on mortality and function following pelvic ring and acetabular injuries".J Bone Joint Surg Am. 2015 Feb 18;97(4):e23. doi: 10.2106/JBJS.N.01190. J Bone Joint Surg Am. 2015. PMID: 25695994 No abstract available.
References
-
- Dalal SA, Burgess AR, Siegel JH, Young JW, Brumback RJ, Poka A, Dunham CM, Gens D, Bathon H. Pelvic fracture in multiple trauma: classification by mechanism is key to pattern of organ injury, resuscitative requirements, and outcome. J Trauma. 1989. July;29(7):981-1000; discussion 1000-2. - PubMed
-
- West JG, Trunkey DD, Lim RC. Systems of trauma care. A study of two counties. Arch Surg. 1979. April;114(4):455-60. - PubMed
-
- West JG, Williams MJ, Trunkey DD, Wolferth CC., Jr Trauma systems. Current status—future challenges. JAMA. 1988. June 24;259(24):3597-600. - PubMed
-
- Mann NC, Mullins RJ, MacKenzie EJ, Jurkovich GJ, Mock CN. Systematic review of published evidence regarding trauma system effectiveness. J Trauma. 1999. September;47(3)(Suppl):S25-33. - PubMed
-
- Mackenzie EJ, Rivara FP, Jurkovich GJ, Nathens AB, Frey KP, Egleston BL, Salkever DS, Weir S, Scharfstein DO. The National Study on Costs and Outcomes of Trauma. J Trauma. 2007. December;63(6)(Suppl):S54-67; discussion S81-6. - PubMed
