

Utility of (18)F FDG-PET/CT for predicting prognosis of luminal-type breast cancer
- PMID: 25697596
- PMCID: PMC4344554
- DOI: 10.1007/s10549-015-3303-9
Utility of (18)F FDG-PET/CT for predicting prognosis of luminal-type breast cancer
Abstract
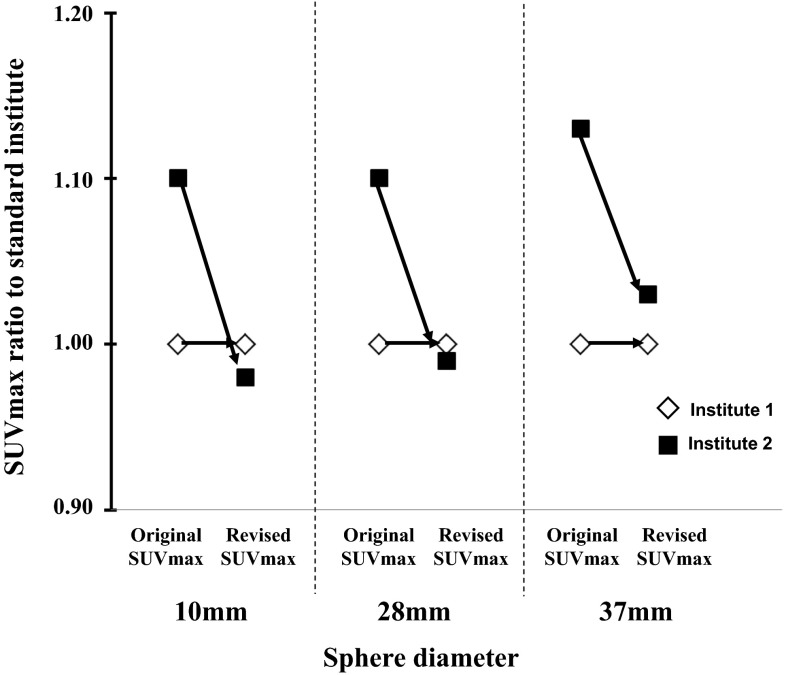
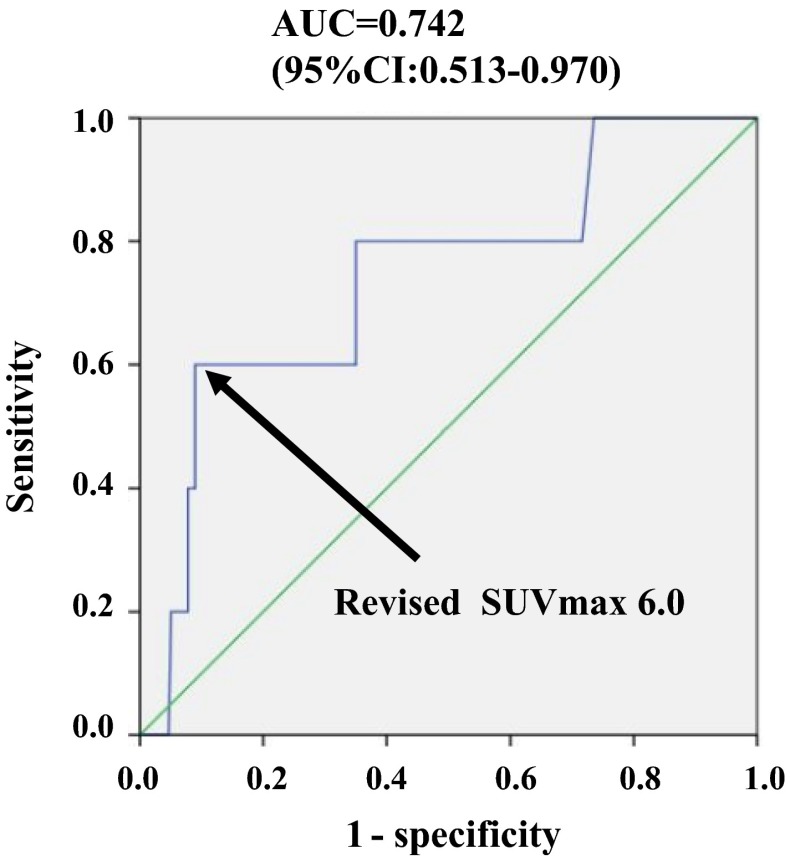
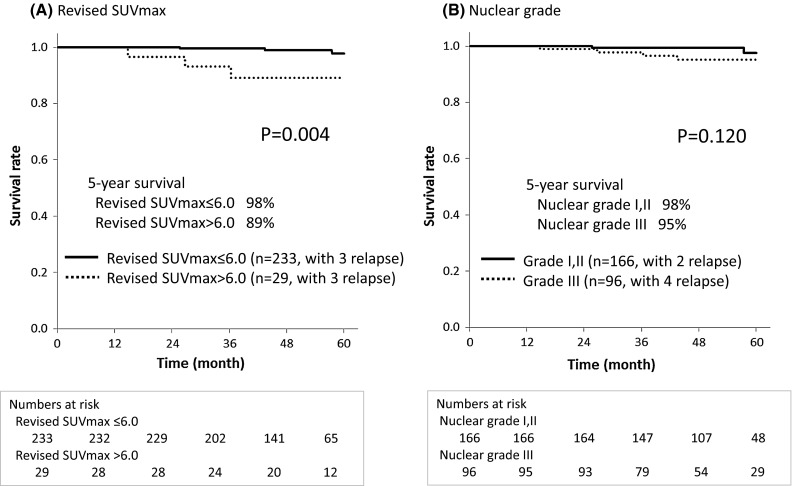
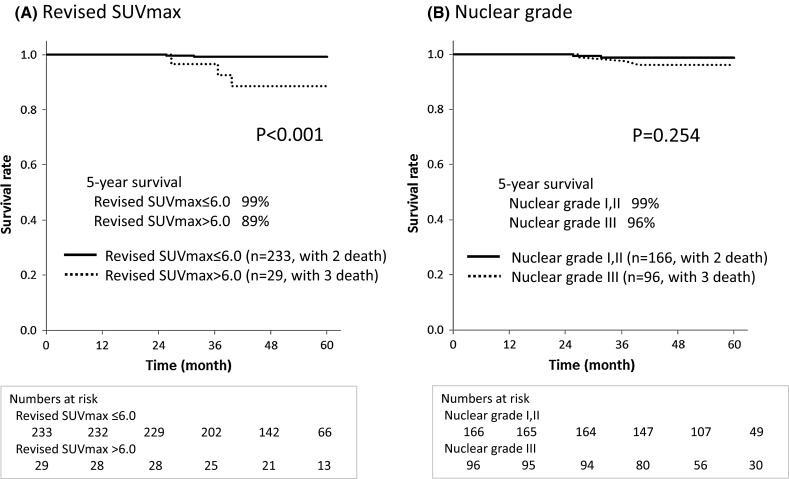
Postoperative prognosis is better for hormonal receptor-positive breast cancer than for other phenotypes; however, there are no definitive predictive factors for relapse or survival. This study aimed to evaluate the maximum standardized uptake value (SUVmax) on (18)F-fluoro-2-deoxy-glucose positron emission tomography/computed tomography (FDG-PET/CT) and clinicopathological characteristics as possible predictors of postoperative relapse-free survival (RFS) and overall survival (OS) in hormonal receptor-positive breast cancer patients. We evaluated 262 patients with Stage I-III breast cancer diagnosed as luminal type (luminal A, 166; luminal B, 96 patients) who underwent preoperative FDG-PET/CT between January 2006 and December 2011 at two institutions. The relationships among SUVmax and clinicopathological factors (age, clinical T/N stage, nuclear grade, lymph node metastasis and vascular invasion) were evaluated. A phantom study was performed to correct differences in PET/CT analysis between two institutions. The patients were divided according to the SUVmax cutoff on receiver operating characteristic (ROC) analysis for OS (≤6.0 group vs. >6.0 group, AUC = 0.742). Clinical T-factor and nuclear grade were significantly correlated with SUVmax (p < 0.0001 and p = 0.0092, respectively). In the uni- and multivariate analyses using the Cox model for relapse, SUVmax was significant (p = 0.013 and p = 0.055, respectively) among characteristics. RFS curves showed that prognosis was significantly better for the SUVmax ≤ 6.0 group than for the SUVmax > 6.0 group (p = 0.004). Similarly, SUVmax was significant for OS (p = 0.007 and p = 0.008). OS was significantly different between the SUVmax ≤ 6.0 and >6.0 groups (p < 0.001). SUVmax was useful for predicting outcomes in patients with luminal-type breast cancer.
Figures
References
-
- Vansteenkiste JF, Stroobants SG, Dupont PJ, De Leyn PR, Verbeken EK, Deneffe GJ, et al. Prognostic importance of the standardized uptake value on (18)F-fluoro-2-deoxy-glucose-positron emission tomography scan in non-small-cell lung cancer: an analysis of 125 cases. Leuven Lung Cancer Group. J Clin Oncol. 1999;17:3201–3206. - PubMed
-
- Okazumi S, Isono K, Enomoto K, Kikuchi T, Ozaki M, Yamamoto H, et al. Evaluation of liver tumors using fluorine—18-fluoro-2-deoxy-d-glucose PET. J Nucl Med. 1992;33:339–344. - PubMed
-
- Fuster D, Duch J, Paredes P, Velasco M, Muñoz M, Santamaría G, et al. Preoperative staging of large primary breast cancer with [18F]fluorodeoxyglucose positron emission tomography/computed tomography compared with conventional imaging procedures. J Clin Oncol. 2008;26:4746–4751. doi: 10.1200/JCO.2008.17.1496. - DOI - PubMed
-
- Okada J, Yoshikawa K, Itami M, Imaseki K, Uno K, Itami J, et al. Positron emission tomography using fluorine-18-fluorodeoxyglucose in malignant lymphoma: a comparison with proliferative activity. J Nucl Med. 1992;33:325–329. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
