

Influence of statin use on the incidence of recurrent venous thromboembolism and major bleeding in patients receiving rivaroxaban or standard anticoagulant therapy
- PMID: 25698905
- PMCID: PMC4334416
- DOI: 10.1186/1477-9560-12-26
Influence of statin use on the incidence of recurrent venous thromboembolism and major bleeding in patients receiving rivaroxaban or standard anticoagulant therapy
Abstract
Background: Statins may reduce the risk of first and recurrent venous thromboembolism (VTE). No data are available on their potential benefit in patients treated with the oral anticoagulant rivaroxaban.
Methods: The EINSTEIN DVT/PE and EINSTEIN Extension studies compared rivaroxaban with standard of care (n=8280) and placebo (n=1188), respectively. The incidences of recurrent VTE and major bleeding per 100 patient-years for exposure (or not) to statins were calculated. A Cox proportional hazards model was constructed, stratified by index event and intended treatment duration, with statin use as a time-dependent variable, for each treatment group (rivaroxaban vs enoxaparin/vitamin K antagonist or placebo) and adjusted for relevant variables.
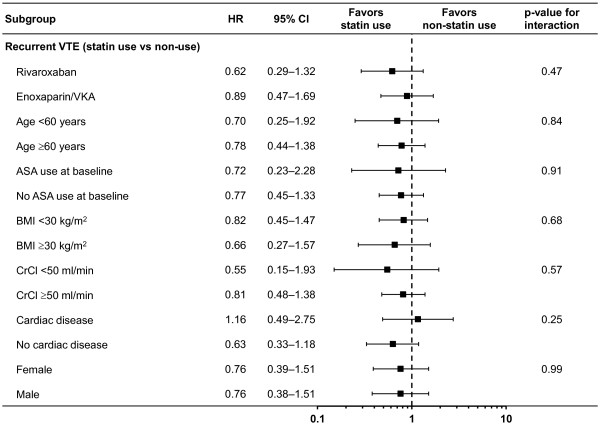
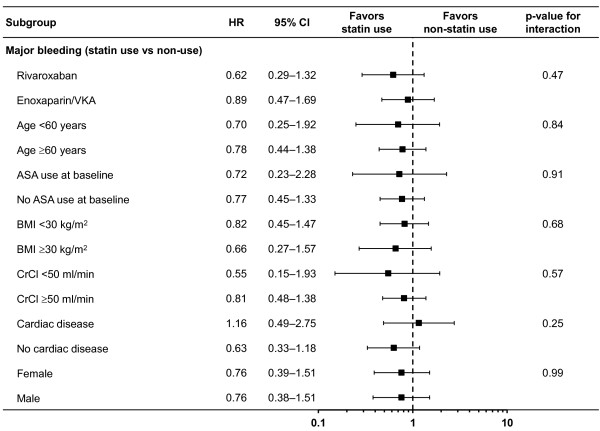
Results: In EINSTEIN DVT/PE, 1509 (18.3%) patients used statins during the at-risk period, and 6731 (81.7%) did not. Overall, 2.6 recurrent VTEs occurred per 100 patient-years with statin use compared with 3.8 per 100 patient-years without statins (adjusted hazard ratio [HR] 0.76; 95% confidence interval [CI] 0.46-1.25). HRs for recurrent VTE were similar for concomitant use of rivaroxaban-statin and enoxaparin/VKA-statin. Major bleeding events occurred in 3.0 per 100 patient-years with statin use compared with 2.3 per 100 patient-years without statins (adjusted HR 0.77; 95% CI 0.46-1.29). Due to adjustments in the Cox regression model, the direction of this HR is in contrast to the crude comparison. In EINSTEIN Extension, no recurrent VTEs occurred with statin use in the rivaroxaban group compared with 1.6 per 100 patient-years without statins. In the placebo group, 12.2 recurrent VTEs occurred per 100 patient-years with statin use compared with 13.2 per 100 patient-years without (adjusted HR 0.81; 95% CI 0.35-1.86).
Conclusions: The effect of statins in this secondary analysis of the EINSTEIN VTE treatment program is consistent with other studies that suggest a reduced risk of recurrent VTE, but conclusive evidence of this benefit is lacking. Statins are simple to use, inexpensive, very safe and do not cause bleeding. Therefore, the potential effect on reducing recurrent VTE, which is in the range of that of acetylsalicylic acid, deserves evaluation in a large randomized trial.
Trial registration number: ClinicalTrials.gov: EINSTEIN PE, NCT00439777; EINSTEIN DVT, NCT00440193; EINSTEIN Extension, NCT00439725.
Keywords: Anticoagulant therapy; Rivaroxaban; Statins; Venous thromboembolism.
Figures
Similar articles
-
Oral rivaroxaban versus enoxaparin with vitamin K antagonist for the treatment of symptomatic venous thromboembolism in patients with cancer (EINSTEIN-DVT and EINSTEIN-PE): a pooled subgroup analysis of two randomised controlled trials.Lancet Haematol. 2014 Oct;1(1):e37-46. doi: 10.1016/S2352-3026(14)70018-3. Epub 2014 Sep 28. Lancet Haematol. 2014. PMID: 27030066
-
Benefit-Risk Assessment of Rivaroxaban in Older Patients With Nonvalvular Atrial Fibrillation or Venous Thromboembolism.Drugs Aging. 2025 May;42(5):469-484. doi: 10.1007/s40266-025-01192-7. Epub 2025 Mar 31. Drugs Aging. 2025. PMID: 40163217 Free PMC article. Clinical Trial.
-
Use of prestudy heparin did not influence the efficacy and safety of rivaroxaban in patients treated for symptomatic venous thromboem-bolism in the EINSTEIN DVT and EINSTEIN PE studies.Acad Emerg Med. 2015 Feb;22(2):142-9. doi: 10.1111/acem.12585. Epub 2015 Feb 9. Acad Emerg Med. 2015. PMID: 25676529 Free PMC article. Clinical Trial.
-
Rivaroxaban: a review of its use in the treatment of deep vein thrombosis or pulmonary embolism and the prevention of recurrent venous thromboembolism.Drugs. 2014 Feb;74(2):243-62. doi: 10.1007/s40265-013-0174-4. Drugs. 2014. PMID: 24430916 Review.
-
The use of rivaroxaban for short- and long-term treatment of venous thromboembolism.Thromb Haemost. 2012 Jun;107(6):1035-43. doi: 10.1160/TH11-12-0859. Epub 2012 Feb 28. Thromb Haemost. 2012. PMID: 22371186 Review.
Cited by
-
Statin use and bleeding risk during vitamin K antagonist treatment for venous thromboembolism: a multicenter retrospective cohort study.Haematologica. 2015 Aug;100(8):e295-8. doi: 10.3324/haematol.2015.127183. Epub 2015 Apr 17. Haematologica. 2015. PMID: 25887499 Free PMC article. No abstract available.
-
Statins Effects on Blood Clotting: A Review.Cells. 2023 Nov 27;12(23):2719. doi: 10.3390/cells12232719. Cells. 2023. PMID: 38067146 Free PMC article. Review.
-
Potential interactions between direct oral anticoagulants and atorvastatin/simvastatin: a cohort and case-crossover study.Br J Gen Pract. 2025 Jun 26;75(756):e466-e473. doi: 10.3399/BJGP.2024.0349. Print 2025 Jul. Br J Gen Pract. 2025. PMID: 39609078 Free PMC article.
-
Statin use and venous thromboembolism in cancer: A large, active comparator, propensity score matched cohort study.Thromb Res. 2017 Oct;158:49-58. doi: 10.1016/j.thromres.2017.08.001. Epub 2017 Aug 10. Thromb Res. 2017. PMID: 28822240 Free PMC article.
-
Statins as a preventative therapy for venous thromboembolism.Cardiovasc Diagn Ther. 2017 Dec;7(Suppl 3):S207-S218. doi: 10.21037/cdt.2017.09.12. Cardiovasc Diagn Ther. 2017. PMID: 29399524 Free PMC article. Review.
References
-
- Rahimi K, Bhala N, Kamphuisen P, Emberson J, Biere-Rafi S, Krane V, Robertson M, Wilkstrand J, McMurray J. Effect of statins on venous thromboembolic events: a meta-analysis of published and unpublished evidence from randomised controlled trials. PLoS Med. 2012;9:e1001310. doi: 10.1371/journal.pmed.1001310. - DOI - PMC - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
