

Comparing characteristics of adverse drug events between older and younger adults presenting to a Taiwan emergency department
- PMID: 25700322
- PMCID: PMC4554176
- DOI: 10.1097/MD.0000000000000547
Comparing characteristics of adverse drug events between older and younger adults presenting to a Taiwan emergency department
Abstract
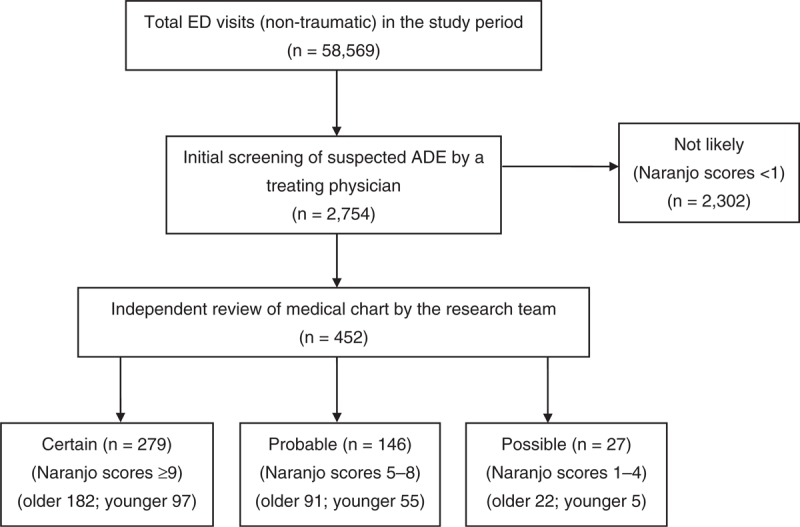
To compare the proportion, seriousness, preventability of adverse drug events (ADEs) between the older adults (≥ 65 years old) and younger adults (<65 years old) presenting to the emergency department (ED), we conducted a prospective observational cohort study of patients 18 years and older presenting to the ED. For all ED visits between March 1, 2009, and Feb 28, 2010, investigators identified ADEs and assessed cases using the Naranjo adverse drug reaction probability scale. Outcomes (proportion, seriousness, and preventability of ADE, length of ED stay, and hospitalization) and associated variables were measured and compared between younger and older adults. The results showed that of 58,569 ED visits, 295 older adults, and 157 younger adults were diagnosed as having an ADE and included in our analysis. The proportion of ADEs leading to ED visits in the older group, 14.3 per 1000 (295/20,628), was significantly higher than the younger group of 4.1 per 1000 (157/37,941). The older group with ADE had a longer ED stay (odds ratio [OR] 3.5, 95% confidence interval [CI] 1.9-6.4 for stay ≥ 24 hours) and larger proportion of preventable ADEs (OR 2.2, 95% CI 1.4-3.6) than the younger group, but there was no significant difference in terms of serious ADEs (OR 0.6, 95% CI 0.3-1.3 for fatal and life threatening) and hospitalization (OR 1.5, 95% CI 0.9-2.6) between the 2 groups. In addition, patients in the older group were more likely to be male, to have symptoms of fatigue or altered mental status, to involve cardiovascular, renal, and respiratory systems, and to have higher Charlson comorbidity index scores, higher number of prescription medications, and higher proportion of unintentional overdose. In conclusion, the proportion of ADE-related ED visits in older adults was higher than younger adults, and many of these were preventable. The most common drug categories associated with preventable ADEs in the older adults were antithrombotic agents, antidiabetic agents, and cardiovascular agents.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Chen YC, Fan JS, Hsu TF, et al. Detection of patients presenting with adverse drug events in the emergency department. Intern Med J 2012; 42:651–657. - PubMed
-
- Hohl CM, Nosyk B, Kuramoto L, et al. Outcomes of emergency department patients presenting with adverse drug events. Ann Emerg Med 2011; 58:270–279.e274. - PubMed
-
- Cohen AL, Budnitz DS, Weidenbach KN, et al. National surveillance of emergency department visits for outpatient adverse drug events in children and adolescents. J Pediatr 2008; 152:416–421. - PubMed
-
- Budnitz DS, Pollock DA, Weidenbach KN, et al. National surveillance of emergency department visits for outpatient adverse drug events. JAMA 2006; 296:1858–1866. - PubMed
-
- Reason B, Terner M, Moses McKeag A, et al. The impact of polypharmacy on the health of Canadian seniors. Fam Pract 2012; 29:427–432. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
