

De novo pulmonary small cell carcinomas and large cell neuroendocrine carcinomas harboring EGFR mutations: Lack of response to EGFR inhibitors
- PMID: 25700797
- PMCID: PMC4355318
- DOI: 10.1016/j.lungcan.2015.02.003
De novo pulmonary small cell carcinomas and large cell neuroendocrine carcinomas harboring EGFR mutations: Lack of response to EGFR inhibitors
Abstract
Introduction: Epidermal growth factor receptor (EGFR) mutations are present in 10-20% of all non-small-cell lung cancers and predict for response to EGFR tyrosine kinase inhibitors (TKIs). However, the incidence of these mutations and their ability to predict response to TKIs in high-grade pulmonary neuroendocrine carcinomas [i.e. small cell lung cancer (SCLC) and large cell neuroendocrine carcinoma (LCNEC)] is unknown.
Methods: The presence of EGFR mutations, clinicopathologic and anti-cancer therapy response data were retrospectively compiled and analyzed from a cohort of 608 patients-lung tumors to identify EGFR mutated high-grade pulmonary neuroendocrine carcinomas. We identified 126 EGFR-mutated (21.8% of 578 successful genotyped cases) lung cancers and only 2 (1.6%) were high-grade neuroendocrine carcinomas.
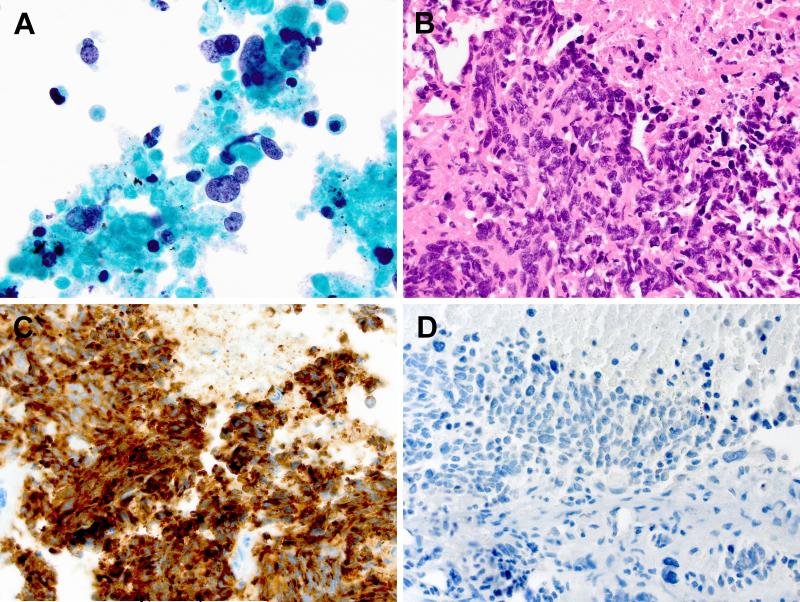
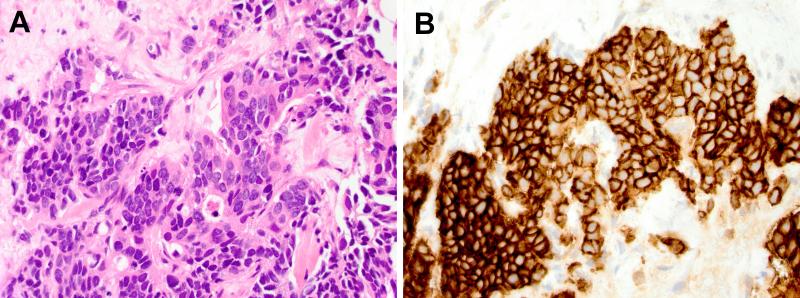
Results: Case one was of a 63 year-old white never smoker woman with extensive stage SCLC harboring EGFR-delL747_P753insS but without EGFR protein expression. After progression on carboplatin/etoposide, the patient was treated with erlotinib and developed progressive disease with a survival <3 months from start of erlotinib. Case two was of a 73 year-old Asian 30 pack-year smoker man with metastatic LCNEC harboring EGFR-delL747_P753insQS and also lacking EGFR protein expression. The patient received first line therapy with erlotinib and had progressive disease with a survival of 4 months.
Conclusions: The lack of response to EGFR TKIs in EGFR mutated de novo SCLC and LCNEC reported here may indicate that tumor differentiation affects tumor dependency on EGFR as a driver oncogene.
Keywords: EGFR; Erlotinib; Large cell neuroendocrine carcinoma; Mutation; Never-smoker; Progression; Resistance; Small cell lung cancer.
Copyright © 2015 Elsevier Ireland Ltd. All rights reserved.
Figures
References
-
- Siegel R, Ma J, Zou Z, et al. Cancer statistics, 2014. CA Cancer J Clin. 2014;64:9–29. - PubMed
-
- Gerber DE, Gandhi L, Costa DB. Management and future directions in non-small cell lung cancer with known activating mutations. Am Soc Clin Oncol Educ Book. 2014:e353–e365. - PubMed
-
- Lindeman NI, Cagle PT, Beasley MB, et al. Molecular Testing Guideline for Selection of Lung Cancer Patients for EGFR and ALK Tyrosine Kinase Inhibitors: Guideline from the College of American Pathologists, International Association for the Study of Lung Cancer, and Association for Molecular Pathology. J Thorac Oncol. 2013;8:823–859. - PMC - PubMed
-
- Zakowski MF, Ladanyi M, Kris MG. EGFR mutations in small-cell lung cancers in patients who have never smoked. N Engl J Med. 2006;355:213–215. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
