

Ionic mechanisms of arrhythmogenesis
- PMID: 25701094
- PMCID: PMC4504834
- DOI: 10.1016/j.tcm.2015.01.005
Ionic mechanisms of arrhythmogenesis
Abstract
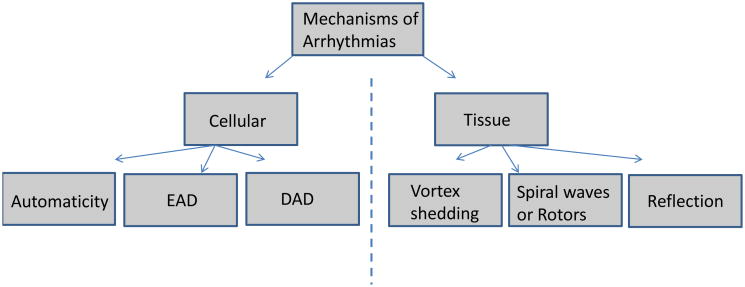
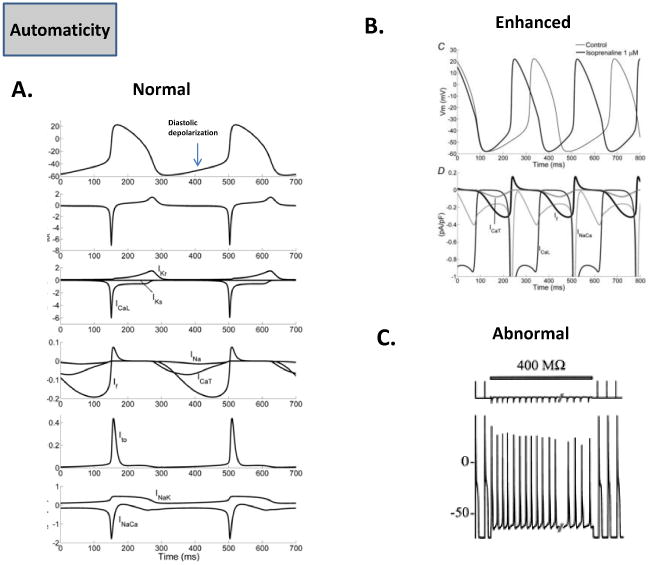
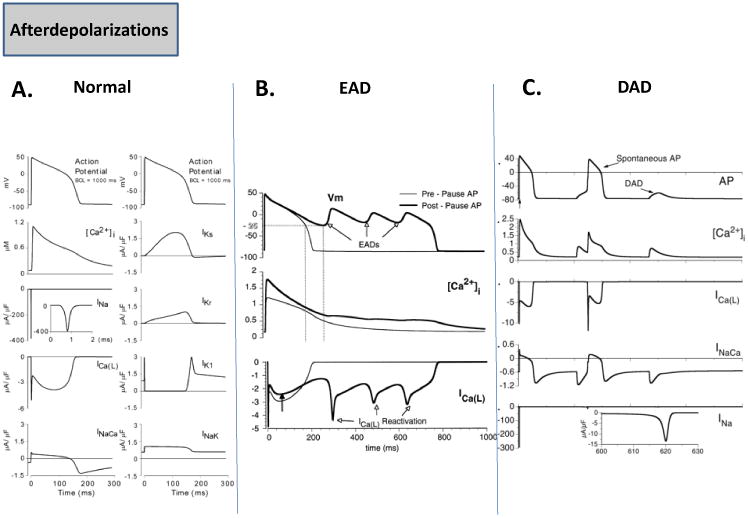
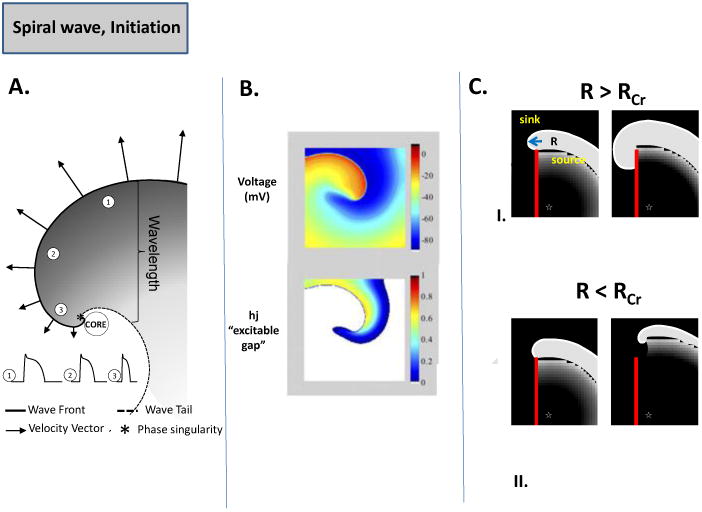
The understanding of ionic mechanisms underlying cardiac rhythm disturbances (arrhythmias) is an issue of significance in the medical science community. Several advances in molecular, cellular, and optical techniques in the past few decades have substantially increased our knowledge of ionic mechanisms that are thought to underlie arrhythmias. The application of these techniques in the study of ion channel biophysics and regulatory properties has provided a wealth of information, with some important therapeutic implications for dealing with the disease. In this review, we briefly consider the cellular and tissue manifestations of a number of cardiac rhythm disturbances, while focusing on our current understanding of the ionic current mechanisms that have been implicated in such rhythm disturbances.
Copyright © 2015 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Channels, arrhythmias, and … the search for the impossible?Trends Cardiovasc Med. 2015 Aug;25(6):497-8. doi: 10.1016/j.tcm.2015.04.014. Epub 2015 Jun 9. Trends Cardiovasc Med. 2015. PMID: 26145202 No abstract available.
References
-
- Heijman J, Voigt N, Nattel S, Dobrev D. Cellular and molecular electrophysiology of atrial fibrillation initiation, maintenance, and progression. Circ Res. 2014 Apr 25;114(9):1483–99. - PubMed
-
- Cerrone M, Cummings S, Alansari T, Priori SG. A clinical approach to inherited arrhythmias. Circ Cardiovasc Genet. 2012 Oct 1;5(5):581–90. Review. - PubMed
-
- Tomaselli GF, Zipes DP. What causes sudden death in heart failure? Circ Res. 2004 Oct 15;95(8):754–63. Review. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
