

Obesity and extent of emphysema depicted at CT
- PMID: 25703460
- PMCID: PMC4444213
- DOI: 10.1016/j.crad.2015.01.007
Obesity and extent of emphysema depicted at CT
Abstract
Aim: To investigate the underlying relationship between obesity and the extent of emphysema depicted at CT.
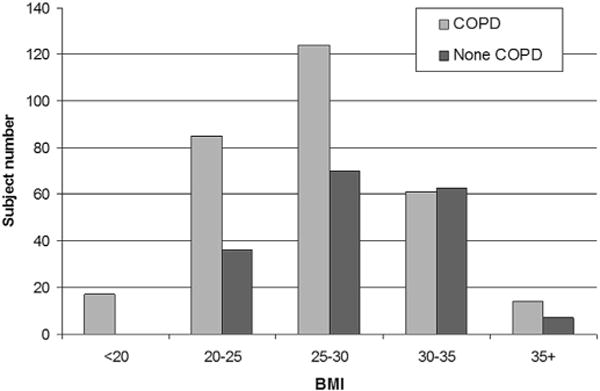
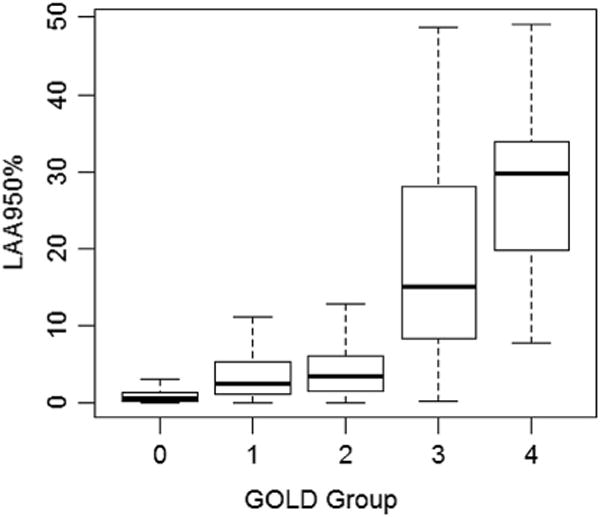
Methods and materials: A dataset of 477 CT examinations was retrospectively collected from a study of chronic obstructive pulmonary disease (COPD). The low attenuation areas (LAAs; ≤950 HU) of the lungs were identified. The extent of emphysema (denoted as %LAA) was defined as the percentage of LAA divided by the lung volume. The association between log-transformed %LAA and body mass index (BMI) adjusted for age, sex, the forced expiratory volume in one second as percent predicted value (FEV1% predicted), and smoking history (pack years) was assessed using multiple linear regression analysis.
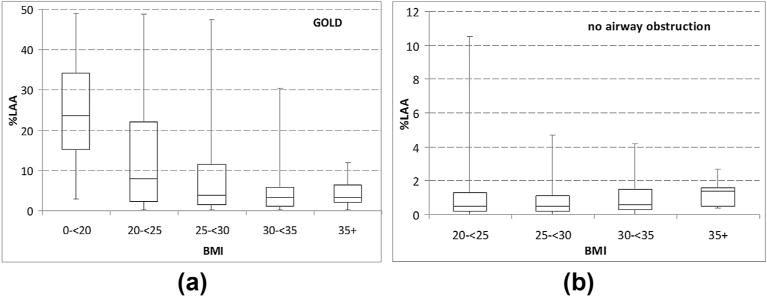
Results: After adjusting for age, gender, smoking history, and FEV1% predicted, BMI was negatively associated with severe emphysema in patients with COPD. Specifically, one unit increase in BMI is associated with a 0.93-fold change (95% CI: 0.91-0.96, p<0.001) in %LAA; the estimated %LAA for males was 1.75 (95% CI: 1.36-2.26, p<0.001) times that of females; per 10% increase in FEV1% predicated is associated with a 0.72-fold change (95% CI: 0.69-0.76, p<0.001) in %LAA.
Conclusion: Increasing obesity is negatively associated with severity of emphysema independent of gender, age, and smoking history.
Copyright © 2015 The Royal College of Radiologists. Published by Elsevier Ltd. All rights reserved.
Figures
Similar articles
-
Identification of occult parechymal disease such as emphysema or airway disease using screening computed tomography.COPD. 2010 Apr;7(2):117-25. doi: 10.3109/15412551003631717. COPD. 2010. PMID: 20397812
-
Impact of emphysema and airway wall thickness on quality of life in smoking-related COPD.Respir Med. 2013 Aug;107(8):1201-9. doi: 10.1016/j.rmed.2013.04.016. Epub 2013 May 25. Respir Med. 2013. PMID: 23711580
-
Impact of emphysema heterogeneity on pulmonary function.PLoS One. 2014 Nov 19;9(11):e113320. doi: 10.1371/journal.pone.0113320. eCollection 2014. PLoS One. 2014. PMID: 25409328 Free PMC article.
-
Decrease in Small Pulmonary Vessels on Chest Computed Tomography in Light Smokers Without COPD: An Early Change, but Correlated with Smoking Index.Lung. 2017 Apr;195(2):179-184. doi: 10.1007/s00408-017-9985-5. Epub 2017 Feb 21. Lung. 2017. PMID: 28224233
-
Does radiographic emphysema correlate with low bone mineral density?Curr Opin Pulm Med. 2012 Mar;18(2):125-30. doi: 10.1097/MCP.0b013e32834f8194. Curr Opin Pulm Med. 2012. PMID: 22273685 Review.
Cited by
-
Sex differences of COPD phenotypes in nonsmoking patients.Int J Chron Obstruct Pulmon Dis. 2016 Jul 22;11:1657-62. doi: 10.2147/COPD.S108343. eCollection 2016. Int J Chron Obstruct Pulmon Dis. 2016. PMID: 27524891 Free PMC article.
-
Dietary ω-6 polyunsaturated fatty acid arachidonic acid increases inflammation, but inhibits ECM protein expression in COPD.Respir Res. 2018 Nov 3;19(1):211. doi: 10.1186/s12931-018-0919-4. Respir Res. 2018. PMID: 30390648 Free PMC article.
-
A machine learning model and identification of immune infiltration for chronic obstructive pulmonary disease based on disulfidptosis-related genes.BMC Med Genomics. 2025 Jan 8;18(1):7. doi: 10.1186/s12920-024-02076-2. BMC Med Genomics. 2025. PMID: 39780155 Free PMC article.
-
A comparative study of chest CT findings regarding the effects of regional dust exposure on patients with COPD living in urban areas and rural areas near cement plants.Respir Res. 2021 Feb 6;22(1):43. doi: 10.1186/s12931-021-01649-4. Respir Res. 2021. PMID: 33549113 Free PMC article.
-
Obesity Impact on Dyspnea in COPD Patients.Int J Chron Obstruct Pulmon Dis. 2024 Jul 22;19:1695-1706. doi: 10.2147/COPD.S450366. eCollection 2024. Int J Chron Obstruct Pulmon Dis. 2024. PMID: 39070800 Free PMC article.
References
-
- Haslam DW, James WP. Obesity. Lancet. 2005;366:1197–209. - PubMed
-
- Finkelstein EA, Trogdon JG, Cohen JW, et al. Annual medical spending attributable to obesity: payer- and service-specific estimates. Health Aff (Millwood) 2009;28:w822–31. - PubMed
-
- Eknoyan G. Adolphe Quetelet (1796–1874)—the average man and indices of obesity. Nephrol Dial Transplant. 2008;23:47–51. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
