

Heterogeneity in tuberculosis pathology, microenvironments and therapeutic responses
- PMID: 25703567
- PMCID: PMC4368385
- DOI: 10.1111/imr.12252
Heterogeneity in tuberculosis pathology, microenvironments and therapeutic responses
Abstract
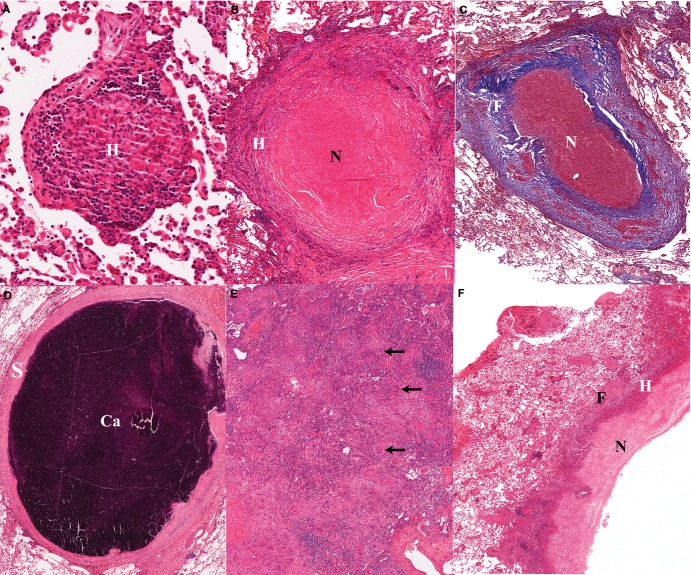
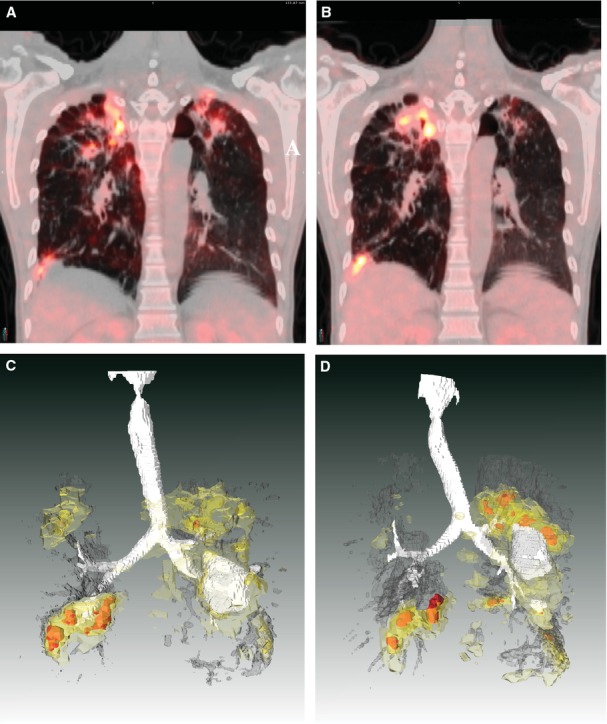
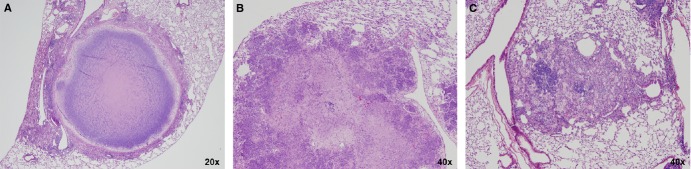
Tuberculosis (TB) lesions are extremely complex and dynamic. Here, we review the multiple types and fates of pulmonary lesions that form following infection by Mycobacterium tuberculosis and the impact of this spatial and temporal heterogeneity on the bacteria they harbor. The diverse immunopathology of granulomas and cavities generates a plethora of microenvironments to which M. tuberculosis bacilli must adapt. This in turn affects the replication, metabolism, and relative density of bacterial subpopulations, and consequently their respective susceptibility to chemotherapy. We outline recent developments that support a paradigm shift in our understanding of lesion progression. The simple model according to which lesions within a single individual react similarly to the systemic immune response no longer prevails. Host-pathogen interactions within lesions are a dynamic process, driven by subtle and local differences in signaling pathways, resulting in diverging trajectories of lesions within a single host. The spectrum of TB lesions is a continuum with a large overlap in the lesion types found in latently infected and active TB patients. We hope this overview will guide TB researchers in the design, choice of read-outs, and interpretation of future studies in the search for predictive biomarkers and novel therapies.
Keywords: animal models; biomarkers; immunopathology; lesion dynamics; tuberculosis.
© 2015 The Authors. Immunological Reviews Published by John Wiley & Sons Ltd.
Figures
References
-
- Barnes DS. The Making of a Social Disease – Tuberculosis in Nineteenth-Century France. Berkeley, Los Angeles, London: University of California Press; 1995.
-
- Canetti G. The Tubercle Bacillus. New York: Springer Publishing COmpany; 1955.
-
- Dannenberg AM., Jr . Pathogenesis of Human Pulmonary Tuberculosis. Washington, DC: ASM Press; 2006.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
